Javadalaemehosp.ir
INTERVENTRICULAR SEPTUM HYDATID CYST: 6- year follow-up
Mirzaie Asadollah M.D, Mirzaie Maryam M.D*
Abstract
Hydatid cyst disease should be considered in differential diagnosis. It can present in nonspecific symptoms especially in the endemic areas. Cardiac involvement should be considered in patients with previous hydatid cyst disease. Cardiac hydatid cysts account for less than 2% of all hydatid diseases. We report the case of a 14-year-old boy with the diagnosis of arterial occlusion of the right lower extremity. Surgical exploration of the femoral artery revealed multiple hydatid cysts. Echocardiography showed a mobile mixed mass lesion. Complete resection of the mass was done from interventricular septum. Post cardiac operative histopathological examination revealed a complicated hydatid cyst confirming complete mass excision. In this case a 6 year clinical and serological tests evaluation follow-up after surgical treatment had showed no evidence of recurrence. This case emphasizes that, in endemic countries, primary cardiovascular echinococcosis should be considered.
Key words: Hydatid Cyst, Interventricular Septum, Femoral Artery Emboli
Hydatidosis due to the cestode Echinococcus granulosus is a disease which has been reported global, but is endemic in Asia, the Middle East, North Africa and Australia, especially it is far more frequent in Mediterranean countries.1, 2 The adult taenia lives in the small intestine of carnivores such as dogs, foxes, and wolves as the main host. Taenia eggs are excreted in the feces of these animals and either directly or by contamination of plants, fruits or vegetables, enters the gut of herbivores where the enzymes dissolve the eggs and the larvae are released. 3The parasite again enters the main host as these contaminated animals are eaten by carni vores.Man is an intermediate or accidental host of this parasite, and is infested by consuming contaminated plants or vegetables, or by contact with dogs.4 Echinococci produce cysts in different organs and tissue. Cardiac hydatid cysts are extremely rare.5, 6 and although patients may remain asymptomatic for many years or have only minor nonspecific symptoms, they are associated with life-threatening complications. Since the cyst grows very slowly the disease is diagnosed with delay.
Case History
In July 2006 a 14-year-old male patient was admitted to our hospital with 3 days history of complained of acute right
lower extremity pain. He lived in rural community and had no past medical or surgical history. Physical examination
demonstrated pallor and absence of the right leg pulse. The right leg was cold and slightly tender. Routine Laboratory
tests were normal. Femoral angiography demonstrated a filling defect in the right common, internal and external iliac
arteries and complete occlusion of external iliac and common femoral arteries with a poor collateral circulation.
Surgical exploration of the femoral artery was done on 18 July 2006, by incision showed an unusual filling defect
expanding the arterial lumen. Cysts were excised and arterial embolectomy was performed.
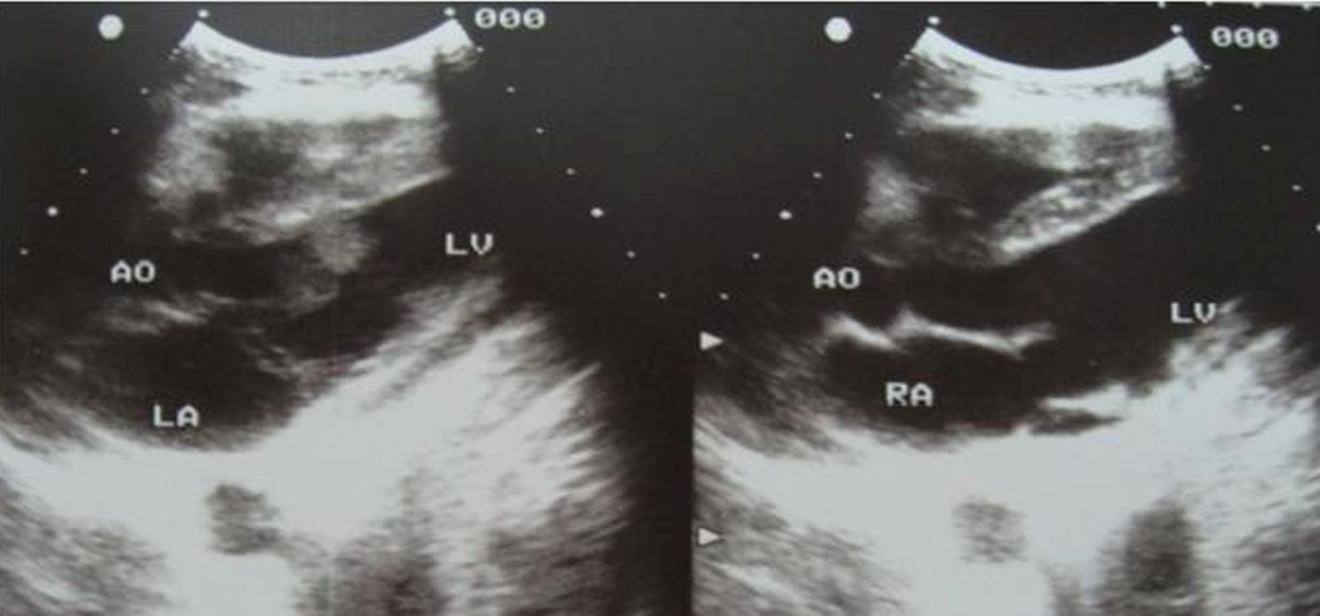
After surgery, the histological investigation showed Hydatid cyst. The patient underwent preoperative chemotherapy administered albendazol at a dose of 10 mg per Kg for 10 days and he also underwent further investigation. Chest radiograph and abdominal CT scan and ultrasonography were normal. No other visceral localization of the disease was found. Echocardiography revealed a mobile mixed mass lesion of 4.0 cm by 3.5 cm in dimension with a 6 mm pedicule(FIGURE 1A,1B), located at the anterior free wall with bulging into the left ventricle. There were no echocardiographic signs of obstruction. An indirect haemagglutination test for E. granulosus was positive. On
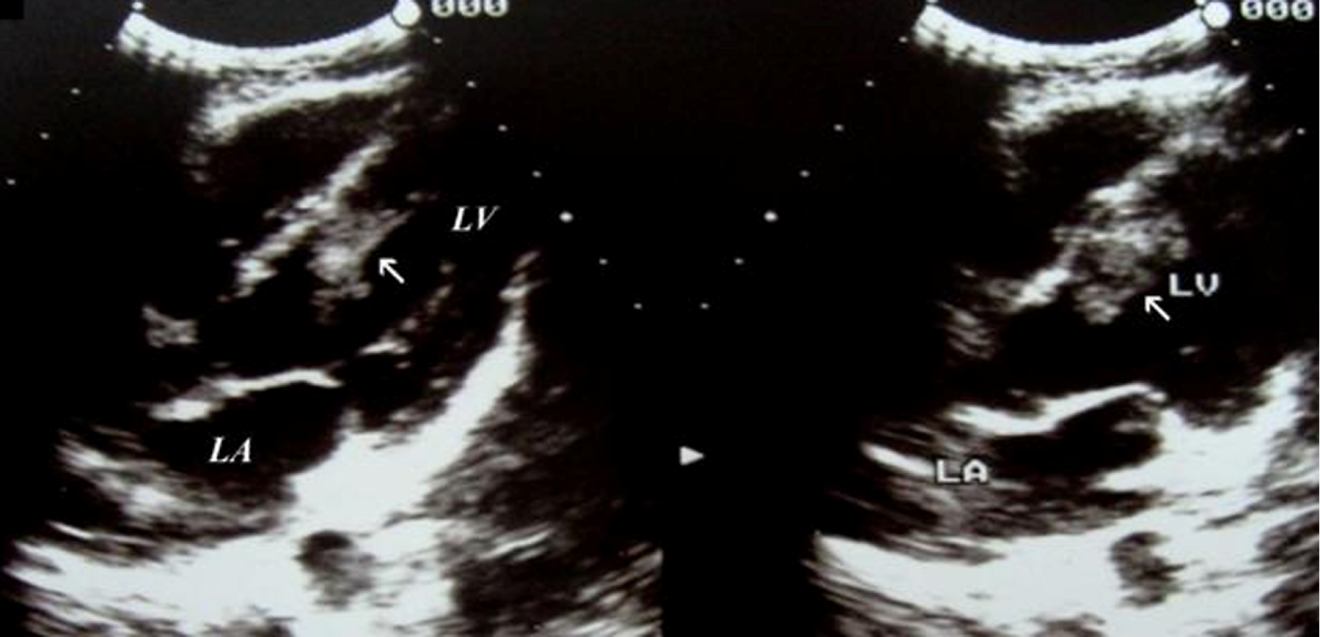
examination, his heart rate was 70 per minute with a blood pressure of 100/60 mmhg. On cardiac auscultation, a low pitched 2/6 systolic murmur was audible at left lower sterna border with no radiation and clear lung fields. His electrocardiogram was normal. The patient underwent cardiac surgery on 1 august 2006 through a median sternotomy and general anesthesia. Cardiopulmonary bypass using bicaval cannulae and an arterial cannula positioned in the ascending aorta. Blood cardioplegia was used. The myocardium was opened and the mass was seen in the interventricular septum and it was totally removed. The cavity had no communication with the ventricular cavities. After complete resection, the cavity closed with primer suturing without felt. Post operative gross and histopathological examination of the excised mass revealed a complicated hydatid cyst confirming complete excision (FIGURE 2A, 2B).The postoperative period was uneventful and the patient was discharged without symptoms. The echocardiogram taken after the operation was normal. He was discharged home 7 days later with a 3-month course of albendazole (200 mg twice daily). the patient was asymptomatic and the the sixth month and one year post operative echocardiography found no further accumulation. The 6 year clinical and serological tests follow-up evaluation had showed no evidence of recurrence.
Discussion
Human hydatidosis is typically due to infection with the canine tapeworm Echinococcus granulosus.4 Hydatid disease
is commonly caused by the parasite E. granulosus. Dogs and other carnivores are the primary host and sheep the
intermediate host, whereas humans are the accidental intermediate host who do not complete the life-cycle of the
parasite. Humans usually become affected by the ingestion of food or milk or water contaminated by dog faeces
containing the ova of the parasite. 3 When a human ingests the eggs, embryos escape from the eggs, penetrate the
intestinal mucosa, and enter the portal circulation. Most are filtered out by the liver or the lungs, but some escape into
the general circulation to involve the brain, kidneys, bones, heart, and other tissues. 4 The diagnosis is usually made
by combination of clinical finding, Imaging and serological tests also a high suspicion and history of exposure in an
endemic area gives clue to the diagnosis.3, 7 Cardiac hydatid cysts accounts for less than 2% of all hydatid diseases.
They most commonly affect the left Ventricle (55–60%), but also the right ventricle, left atrium (8%), pulmonary artery,
pericardium (7–8%) and the interventricular septum (5–9%). The clinical presentation of cardiac hydatid disease is
variable and the diagnosis is difficult. Since cystic mass grows slowly, it is usually asymptomatic or can produce
atypical or mild symptoms depending on localization; however, rupture of the hydatid cysts may induce embolism or
life-threatening anaphylactic shock.5, 8 when the interventricular septum is involved Complications such as
anaphylaxis and embolisation into pulmonary and systemic sites can occur. 6 Early diagnosis of this condition is
crucial to avoid these complications. In our case the unusual presentation revealed femoral embolisation caused by
interventricular septum. Imaging indicated left ventricular septum as a probable primary site for ileofemoral artery
location. Surgical treatment is the only option for cardiac hydatid disease since medical therapy does not offer
insurance against rupture of the cyst and its potential complications. 3, 1 Resection of an intracardiac cyst is
recommended to avoid the grave complication of rupture, which is as common as 39 %. 3, 2
In our case, the hydatid cyst was located in the interventricular septum. The importance of our case rests in the unusual location of the hydatid cysts and also it's unusual presentation. In such cases, differential diagnosis should include cardiac tumors, thrombus, myxoma and other rare intracardiac tumors, such a sarcoma. Recurrence has been reported in 10% of patients undergoing hydatid cyst surgery due to spillage of protoscoleces 9, 10.In this case a 6 year clinical and serological tests evaluation follow-up had showed no evidence of recurrence. This case emphasizes that, in endemic countries, primary cardiovascular echinococcosis should be considered in the differential diagnosis and conditions.
References
1.Eylem Tuncer, Serpil Gezer Tas,Ilker Mataraci, Altug Tuncer, Arzu Antal Donmez, Mehmet Aksut,et al. Surgical Treatment of Cardiac Hydatid Disease in 13 Patients. Tex Heart Inst J 2010; 37(2):189–93.
2. Hafize Yaliniz AT, Orhan K. Salih, Tumer Ulus.Surgical Treatment of Cardiac Hydatid Disease A Report of 7 Cases. J Thorac Cardiovasc Surg 2006; 33(3):333–9.
3. Kamath SM, Mysorekar VV, Rao SG, Varma RG. Intraventricular hydatid cyst in a child. Indian J Pathol Microbiol 2009; 52(4):571-2.
4.Polat P, Kantarci M, Alper F, Suma S, Koruyucu MB, Okur A. Hydatid disease from head to toe. Radiographics 2003; 23:475–94.
5. Elangovan S HK, Meenakshi K, Swaminathan, TS MP. Left ventricular hydatid cyst with myocardial infarction in a patient with severe rheumatic mitral stenosis. Indian Heart J 2004; 56:664–7.
6.Erentug , Bozbuga N, Kirali K, Mataraci I, Kaymaz C, Balkanay M, et al. Cardiac hydatid cysts: surgical treatment and results. J Card Surg 2004; 19(4):358–60.
7. S K Muthu AT, S Govindarajan, C M A Coutinho, W J Gunawardena, T S Swaminathan. Hydatid cyst of the cardiac interventricular septum: report of two cases. British Journal of Radiology 2007; 80:278-82.
8. Hong Bin Wang ML, Hao Wen Isolated Cardiac Hydatid Cyst. Journal of Cardiac Surgery 2010; 25(6):702–3.
9. Ameli M, Mobarhan HA, Nouraii SS. Surgical treatment of hydatid cysts of the heart: report of six cases. J Thorac
Cardiovasc Surg 1989; 98:892–901.
10. Rasheed A Saad, Khalid MA Amer, Marcello Migliore, Tarek Aziz, Ahmed Azzu. Right Intraventricular Hydatid Cyst of the Heart. Asian Cardiovascular Thorac Ann 2003; 11:160–2.
Source: http://javadalaemehosp.ir/LinkClick.aspx?fileticket=O7B2rYut9lM%3D&tabid=567
iNterView mit harjeeV kaNdhari / aL dobowi group / iNfiNity tyres"The German market is a very important market for us" The still-young tyre brand Infinity Tyres is securing more and more market shares on an international scope. We spoke to the Executive Director of the Al Dobowi Group, Harjeev Kandhari, about Infinity´s company philosophy, the importance of networks among partners and the challenges Infinity has to face due to the legal requirements of specific tyre designations.
This electronic representation of FoxP2 Media LLC/The Medical Roundtable intellectual property is provided for noncommercial use only. Unauthorized posting of FoxP2 Media LLC/The Medical Roundtable electronic documents to a non-FoxP2 Media LLC website is prohibited. Prior written permission is required from FoxP2 Media LLC to reproduce, or reuse in another form, any of our documents for commercial use.