Rph.wa.gov.au


Malaria resources
Division of Laboratory Medicine
Royal Perth Hospital

Contents

History
Malaria is a protozoal disease transmitted by the Anopheles mosquito, caused
by minute parasitic protozoa of the genus Plasmodium, which infect human and
insect hosts alternatively. It is a very old disease and prehistoric man is
thought to have suffered from malaria. It probably originated in Africa and
accompanied human migration to the Mediterranean shores, India and South
East Asia. In the past it used to be common in the marshy areas around Rome
and the name is derived from the Italian, (mal-aria) or "bad air"; it was also
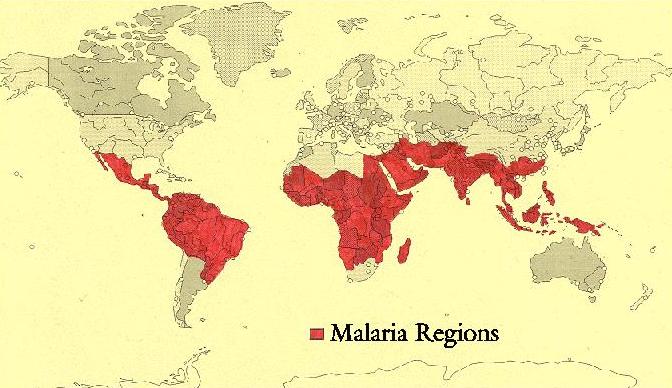
known as Roman fever. Today some 500 hundred million people in Africa,
India, South East Asia and South America are exposed to endemic malaria and
it is estimated to cause two and a half million deaths annually, one million of
which are children.
Fishermen and traders, long before British colonisation, probably introduced the
disease into northern Australia and in the past malaria was not uncommon in
the northern parts of the country. In Western Australia an explosive outbreak of
falciparum malaria occurred at Fitzroy Crossing in 1934 which at first was
mistaken for influenza and resulted in 165 deaths. WHO declared Australia
free of malaria in 1981, however since that time 9 patients have contracted
locally acquired malaria.
The so called "airport malaria" has become a problem in recent years. A
publican working in an establishment close to London's Heathrow Airport
became acutely ill and was found to be suffering from falciparum malaria; he
had never been out of the country. A lady driving her car past the same airport
became ill with malaria although she too had never been out of the country.
Four workers unloading a cargo plane at Amsterdam airport became infected
with malaria. It is assumed that infected mosquitoes were carried on planes
from Africa and released at the destination airport.
World distribution of Malaria

While it was recognised that the Anopheles mosquito played a key role in the transmission of the disease, it was not until 1948 that all the stages in its life cycle were identified. The parasite undergoes a development stage in the mosquito and the female of the species requires a blood meal to mature her eggs. She bites a human and injects material from her salivary glands, which contains primitive malarial parasites called sporozoites, before feeding. These sporozoites circulate in the blood for a short time and then settle in the liver where they enter the parenchymal cells and multiply; this stage is known as pre-erythrocytic schizogony. After about 12 days there may be many thousands of young parasites known as merozoites in one liver cell, the cell ruptures and the free merozoites enter red blood cells. The blood stages of the four species of malaria can be seen in the section on In the case of P. vivax, and P.ovale the liver cycle continues and requires a course of primaquine to eliminate it. P.falciparum on the other hand does not have a continuing liver cycle. In the red blood cells the parasites develop into two forms, a sexual and an asexual cycle. The sexual cycle produces male and female gametocytes, which circulate in the blood and are taken up by a female mosquito when taking a blood meal. The male and female gametocytes fuse in the mosquito's stomach and form oöcysts in the wall of the stomach. These oöcysts develop over a period of days and contain large numbers of sporozoites, which move to the salivary glands and are ready to be injected into man when the mosquito next takes a meal. In the asexual cycle the developing parasites form schizonts in the red blood cells which contain many merozoites, the infected red cells rupture and release a batch of young parasites, merozoites, which invade new red cells. In P.vivax, P.ovale and probably P.malariae, all stages of development subsequent to the liver cycle can be observed in the peripheral blood. However, in the case of P.falciparum only ring forms and gametocytes are usually present in the peripheral blood. Developing forms appear to stick in the blood vessels of the large organs such as the brain and restrict the blood flow with serious consequences. While all four species have a haemolytic component ie. when a new brood of parasites break out of the red blood cell, this is usually of little consequence. The exception is falciparum malaria where the parasites multiply very rapidly and may occupy 30% or more of the red blood cells causing a very significant level of haemolysis. One reason for this is that P.falciparum invades red cells of all ages whereas P.vivax and P.ovale prefer younger red cells, while P.malariae seeks mature red cells.

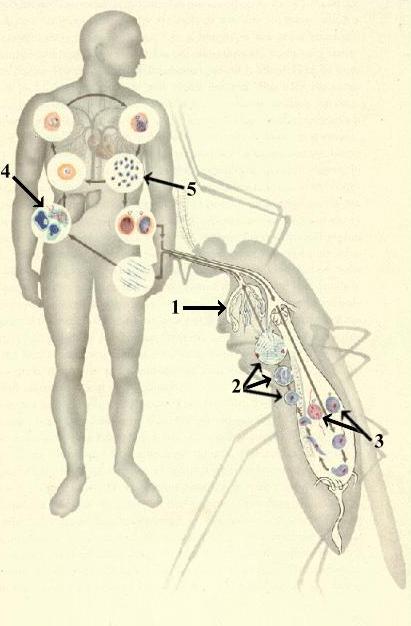
Lifecycle of the malarial parasite
1. Sporozoites in salivary gland.
2. Oöcysts in stomach wall.
3. Male and female gametocytes.
5. Release of merozoites from liver.
These enter red cells where both sexual and asexual cycles continue.
Section of mosquito
showing oöcysts (1)
and sporozoites (2)
Section of liver
showing a greatly
enlarged
parenchymal cell full
of merozoites (see
arrow).
Section of brain
showing blood
vessels blocked with
developing P.
falciparum parasites
(see arrows).
History of Treatment and Prophylaxis
Antimalarial drugs fall into several chemical groups and it is useful to have
some knowledge of their chemistry. The aim here is to give a brief outline of
anti-malarial drugs and their usefulness today, when drug resistant strains of
malaria have become a major problem. It is not a comprehensive history nor
does it include a number of drugs which are no longer used.
Quinine has been used for more than three centuries and until the 1930's it was the only effective agent for the treatment of malaria. It is one of the four main alkaloids found in the bark of the Cinchona tree and is the only drug which over a long period of time has remained largely effective for treating the disease. It is now only used for treating severe falciparum malaria partly because of undesirable side effects. In Africa in the 1930's and 40's it was known for people to take quinine when they thought they had "a touch of malaria" and the association of repeated infections with falciparum malaria and inadequate treatment with quinine, resulted in the development in some of acute massive intravascular haemolysis and haemoglobinuria ie. black water fever.
Atebrin (mepacrine)
This drug is a 9-amino-acridine developed in the early 1930's. It was used as a prophylactic on a large scale during the Second World War (1939-45) and was then considered a safe drug. It had a major influence in reducing the incidence of malaria in troops serving in South East Asia. It is now considered to have too many undesirable side effects and is no longer used.
Chloroquine
A very effective 4-amino-quinoline both for treatment and prophylaxis. It was first used in the 1940s shortly after the Second World War and was effective in curing all forms of malaria, with few side effects when taken in the dose prescribed for malaria and it was low in cost. Unfortunately most strains of falciparum malaria are now resistant to chloroquine and more recently chloroquine resistant vivax malaria has also been reported.
Proguanil
This drug falls into the biguanide class of antimalarials and was first synthesised in 1946. It has a biguanide chain attached at one end to a chlorophenyl ring and it is very close in structure to pyrimethamine. The drug is a folate antagonist and destroys the malarial parasite by binding to the enzyme dihydrofolate reductase in much the same way as pyrimethamine. It is still used as a prophylactic in some countries.
Malarone
In 1998 a new drug combination was released in Australia called Malarone. This is a combination of proguanil and atovaquone. Atovaquone became available 1992 and was used with success for the treatment of Pneumocystis carrinii. When combined with proguanil there is a synergistic effect and the combination is at the present time a very effective antimalarial treatment. The drug combination has undergone several large clinical trials and has been found to be 95% effective in otherwise drug resistant falciparum malaria. How long it will be before resistant strains of malaria appear remains to be seen. It has been claimed to be largely free from undesirable side effects but it should be noted that proguanil is an antifolate. This is not likely to be a problem with a single treatment course of the drug but some caution should be exercised when using it for prophylaxis. At present it is a very expensive drug.
Maloprim
A combination of dapsone and pyrimethamine. Resistance to this drug is now widespread and its use is no longer recommended.
Fansidar
This is a combination drug, each tablet containing sulphadoxine 500mg. and pyrimethamine 25mg. It acts by interfering with folate metabolism. Resistance to Fansidar is now widespread and serious side effects have been reported. It is no longer recommended.
Mefloquine (Lariam)
First introduced in 1971, this quinoline methanol derivative is related structurally to quinine. The compound was effective against malaria, resistant to other forms of treatment when first introduced and because of its long half life was a good prophylactic, but widespread resistance has now developed and this together with undesirable side effects have resulted in a decline in its use. Because of its relationship to quinine the two drugs must not be used together. There have been reports of various undesirable side effects including several cases of acute brain syndrome, which is estimated to occur in 1 in 10,000 to 1 in 20,000 of the people taking this drug. It usually develops about two weeks after starting mefloquine and generally resolves after a few days.
Halofantrin (Halfan)
This belongs to a class of compound called the phenanthrene-methanols and is not related to quinine. It is an effective antimalarial introduced in the 1980s, but due to its short half life of 1 to 2 days, is therefore not suitable for use as a prophylactic. Unfortunately resistant forms are increasingly being reported and there is some concern about side effects. Halofantrin has been associated with neuropsychiatric disturbances. It is contraindicated during pregnancy and is not advised in women who are breastfeeding. Abdominal pain, diarrhoea, puritus and skin rash have also been reported.
This is derived from a Chinese herbal remedy and covers a group of products. The two most widely used are artesunate and artemether. While they are widely used in Southeast Asia they are not licensed in much of the so called "Western World", including Australia. A high rate of treatment failures has been reported and it is now being combined with mefloquine for the treatment of falciparum malaria.
Diagnosis
Laboratory Diagnosis
There are four species of the genus plasmodium responsible for the malarial
parasite infections that commonly infect man, P.falciparum, P.vivax, P.malariae
and P.ovale. The most important of these is P.falciparum because it can be
rapidly fatal and is responsible for the majority of malaria related deaths.
Malaria occurs in most tropical regions of the world with P.falciparum
predominating in Africa, New Guinea and Haiti. P.vivax is more common on
the Indian sub-continent and Central America with the prevalence of these two
infections roughly equal in Asia, Oceania and South America. P. malariae is
found in most endemic areas especially sub-Saharan Africa but much less
frequently. P. ovale is relatively unusual outside Africa although some cases
are now being identified in other regions (eg. Southern States of India). It is
also important to recognise that with the relative ease and speed of modern
travel and migration, "imported" cases of malaria may present in any country.
Additionally so called "airport malaria" (see History section) has now been
identified in a number of countries including the USA, UK, Belgium, and
Switzerland. Airport malaria is particularly dangerous since Clinicians may
have little reason to suspect it, if the patient has had no recent travel to areas
where malaria is endemic. This may result in a delay before the correct
diagnosis is made and which may lead to death before appropriate treatment
can be initiated. Small outbreaks of malaria may occur in countries considered
free of the disease, such outbreaks are most likely the result of an infected
person entering the country asymptomatic and where suitable mosquito vectors
are present.
In recent years a number of new techniques based on the "dipstick" format,
have become available for the diagnosis of malaria. These include the ICT-
Malaria Pf, OptiMALr and the Kat-Quick kits. The methods are based on the
principle of the detection of plasmodial histidine rich protein-2 (HRP-2) or
parasite-specific lactate dehydrogenase (pLDH) which is present in
P.falciparum infections. A number of reports claim sensitivities and specificities
approaching 100% while other reports have claimed up to 6% cross reactivity
with sera positive for rheumatoid factor. Some of these "dipstick" methods
have been extended to include screening for other forms of malaria but to date
results have not been quite so impressive.
Dipstick tests have the potential of enhancing the speed and also the accuracy of diagnosing P. falciparum, particularly in non-specialised laboratories where inexperienced or junior staff may be involved, since very little training is required for these techniques. In this laboratory we have found the dipstick kits to be very useful screening or confirmatory tests, especially when there is difficulty in identifying scanty ring forms in blood films. They have proved to be particularly useful out of hours when junior, less experienced staff have been on duty. However dipstick methods are unable to indicate parasite load and in some countries the cost may be prohibitive. A potential problem with these methods is that the circulating antigen may be detected for many days (up to 2 weeks in our laboratory) after the elimination of viable parasites from the circulation. It must therefore be remembered that a positive test may not always be due to an active infection. We would like to emphasise, that we regard these dipstick methods as useful additional tests to the long established method of examining thick and thin blood films (outlined below), which is still regarded as the "gold standard", NOT as replacement methods. The highest density of malaria occurs in countries least able to afford sophisticated and expensive diagnostic tools. Antibodies to malaria can be detected using enzymatic immunoassays or immunofluorescence techniques. The antibodies to the asexual blood stages appear days to weeks after the infection and may persist for months. Although useful in survey work or for screening blood donors and reducing wastage, they are of little value in the "acute" malaria situation. (Vox Sanguinis. 73(3):143-8, 1997. Clin & Exp Immunol. 54(1):127-34, 1983.) Other methods include the QBC II System, Becton-Dickinson's Quantitative Buffy Coat (QBC) method. This involves centrifuging the patient's blood in special capillary tubes precoated with Acridine Orange (AO) in which parasite DNA is stained with AO. A small precision moulded plastic float presses the parasitised red cells (which occupy the upper most part of the red cell column) against the wall of the tube, where they can be viewed by ultra violet light microscopy. The sensitivity of this method is claimed to be very high with experienced users, although some reports suggest that young trophozoites of P. falciparum and P. vivax, could not be distinguished with any degree of certainty and that confirmatory blood films should always examined. Additionally special equipment is required, which may preclude the method from being used in smaller centres. (J Trop Med & Hygene. 96(4):245-8, 1993-Aug)
Another relatively new method is the polymerase chain reaction (PCR) which uses a non-isotopically labelled probe following PCR amplification. It is possible to detect <10 parasites per 10uL of blood and PCR may yet prove to be a valuable addition to the examination of blood films for the diagnosis and speciation of malaria (Am J Trop Med & Hyg. 65(4):355-363. 2001-Oct). Once again the special equipment required precludes all but the larger centres. Some researchers have claimed that PCR (and Elisa) techniques are as sensitive as blood films, however they are infinitely more expensive, require specialised equipment and take a longer time to complete. Examination of a thick blood film should be the first step since this has the advantage of concentrating the parasites by 20 fold in comparison to a thin film, although the parasites may appear distorted making species identification difficult. If parasites are seen then the species should be confirmed by the examination of a thin film. Ideally blood should be collected when the patient's temperature is rising.
Preparation of thick and thin blood films
Thick films
Place a drop of blood in the middle of a clean microscope slide and with the corner of a second slide spread the drop until it is about 10-15mm in diameter. The thickness should be such that it is just possible to see news print through it.
Thin films
Thin films are made in the standard manner. Allow the films to dry, do not leave on the bench in a laboratory which is not fly proofed otherwise the film will be eaten.
When the films are dry, fix and stain the thin films in the conventional manner but be careful about the pH of the stain, a slightly alkaline stain is recommended (pH 7.2) as an acid stain may fail to show the parasites. When only a few thick films are to be stained it is best to use dilute Giemsa stain (1/20), using a staining jar so that the film is in an upright position, this will allow any debris to fall to the bottom of the jar. Do not fix the sample prior to staining. Stain for about 30 minutes, wash gently with clean water and allow to dry. If available use a positive control. When a large number of thick films require staining, Field's stain is preferred because it is very quick. Field's stain comprises two solutions; a polychrome methylene blue (A) and eosin (B). The solutions are kept in covered staining jars.
1. Dip the dry but unfixed film into solution A for 1 or 2 seconds. 2. Remove from solution A and immediately rinse in clean water (a 250ml
beaker with water gently flowing into it is suitable).
3. Dip the film into solution B for 1 or 2 seconds. 4. Rinse in clean water for a few seconds. 5. Place in a vertical position to dry.
If films are old or too thick the red cells may not lyse completely in the brief
staining time. If this is likely dip the film in clean water for a few seconds or
until the haemoglobin has dispersed before staining. Instructions for preparing
Field's stain can be found in many laboratory text books.
Under the microscope examine the thick film first, using an oil immersion or
high dry lens to determine if parasites are present. Be aware of the patient's
platelet and leucocyte counts. Malaria is usually associated with a normal or
reduced leucocyte numbers. A leucocytosis is only found in terminal cases.
Platelet numbers are moderately or markedly reduced in some 80% of patients
with malaria. Parasites may appear distorted if the patient has been treated or
has had inadequate or ineffective prophylaxis.
Mixed infections are not uncommon.
Characteristics of the four species
P. Falciparum
Diagnostic Points
1. Red Cells are not enlarged. 2. Rings appear fine and delicate and there may be several in one cell. 3. Some rings may have two chromatin dots. 4. Presence of marginal or applique forms. 5. It is unusual to see developing forms in peripheral blood films. 6. Gametocytes have a characteristic crescent shape appearance.
However, they do not usually appear in the blood for the first four weeks of infection.
7. Maurer's dots may be present.
Diagnostic Points
1. Red cells containing parasites are usually enlarged. 2. Schuffner's dots are frequently present in the red cells as shown
3. The mature ring forms tend to be large and coarse. 4. Developing forms are frequently present.
P. Malariae
Diagnostic Points
1. Ring forms may have a squarish appearance. 2. Band forms are a characteristic of this species. 3. Mature schizonts may have a typical daisy head appearance with up
to ten merozoites.
4. Red cells are not enlarged. 5. Chromatin dot may be on the inner surface of the ring.
Diagnostic Points
1. Red cells enlarged. 2. Comet forms common (top right). 3. Rings large and coarse. 4. Schuffner's dots, when present, may be prominent. 5. Mature schizonts similar to those of P. malariae but larger and more
Prophylaxis
Antimalarial drug prophylaxis is a difficult area with a number of drug resistant
strains of P. falciparum now common, particularly in South East Asia and
increasingly in Africa. Resistance to Fansidar, Chloroquine, Maloprim, Lariam
and Halofantrine, Malarone and quinine have all been reported. Resistance is
important because falciparum malaria can be rapidly fatal. The type of
prophylaxis used depends on the area being visited (e.g. country, city, rural
area) and local parasite drug resistance patterns.
Pregnant women are especially vulnerable to malaria, which remains an
important cause of stillbirths, infant mortality and low birth weight. Pregnant
women are twice as attractive to malaria-carrying mosquitoes as non-pregnant
women, perhaps due to a greater volume of exhaled air (21%) and a warmer
(0.7°C) skin surface.
Chloroquine offers little or no protection against P. falciparum in South East
Asian countries and this is increasingly the case in other regions. While
effective in suppressing P. falciparum in some parts of Africa and most strains of
P. vivax, resistant forms of P.vivax are appearing and have been reported in
Papua New Guinea, Indonesia, Thailand and India. Combination
chemoprophylaxis such as with chloroquine and FansidarTM is not
recommended because of the potential for greater adverse clinical effects
(including Stevens-Johnson syndrome) and reduced compliance.
It is recommended that travellers commence taking prophylaxis at least a week
before visiting a malaria endemic region so that any adverse drug reactions can
be observed prior to travel. In some cases, this will also allow effective blood
levels to be achieved. The major problem is how best to suppress malaria in
travellers, particularly those visiting regions where it is known that drug-
resistant strains are present. At present the following is recommended:
Travellers should take active measures to protect themselves against mosquito bites. This is the best and most effective means of avoiding malaria. Generally mosquitoes start feeding at dusk. Therefore, there need be no restrictions on dress during the day but, from just before dusk, clothing should be worn that covers the arms and legs. In addition, a mosquito repellent should be applied on other exposed parts. Suitable repellents are "Muskol" and "RID". Both have a high N,N-diethyl-meta-toluamide (DEET) content (more than 15%) which is the active agent. Both are available from retail chemists. Repellents containing more than 30% DEET are not generally recommended.
Care should be taken when using these repellents on children, because serious side effects, sometimes related to excess use, have been reported. DEET-containing repellents can be applied to a child's clothing rather than the skin but it is important to advise parents to wash the child's hands on entering a screened area. If wearing very thin clothing, lightly spray the clothing with repellent because mosquitoes may bite through thin clothing. Knock-down sprays, mosquito coils and pyrethrin-impregnated mosquito nets can also be effective at minimizing vector contact.
Four regimens are set out below. The choice depends on the countries which are to be visited and possible drug sensitivity of the traveller.
Chloroquine
Chloroquine can still be used in some regions but is of limited value in many parts of the world. Treatment should be started one week before travelling to, and continued for four weeks after leaving a malaria endemic area. (Adult dose 300mg weekly taken with a meal, at the same time and on the same day each week). It will suppress but not cure an infection with P. vivax and symptoms may not appear for weeks or months after the traveller has returned home. For children the dose is 5mg/kg base given once a week on the same day each week. Since liquid suspensions for children are no longer available, a tablet has to be divided to provide the appropriate dose. Chloroquine has a bitter taste and should be given to children crushed in a strong flavoured (sweet) drink. Prophylactic drugs in children should not be given without advice from a medical practitioner, preferably one practising from a health travel medical centre. Chloroquine is considered a safe drug for pregnant and lactating women and also for children. However, it is wise to discourage women who are pregnant from travelling to areas where malaria is present because of the difficulties associated with treatment and the risk to the mother and foetus should they get malaria.
Doxycycline
Doxycycline is a suitable prophylactic anti-malarial agent to use in high risk areas such as South East Asia. It must not be used in children under 8 years of age nor in pregnant or breast-feeding women. Doxycycline may cause contraceptive pills to be less effective so additional precautions should be taken. It may cause thrush in some women but usually only when taken for long periods. It may cause severe skin photosensitivity in some individuals. Doxycycline - Adult dose 100mg daily. Start 1-2 days before travelling to a malarious area and continue for 2-4 weeks after leaving. To ensure that the patient is not sensitive to doxycycline it is worthwhile starting treatment 7 days before travelling. It is recommended that it is not taken for longer than three months without a medical review.
Mefloquine (Lariam)
Mefloquine (Lariam) is still a widely used prophylactic. It has a long half life and the convenience of a once weekly dose. For adults (more than 45 kg bodyweight) the dose is 250mg base weekly, starting one week before arrival in a malarious area. Side effects have been reported which are generally mild (e.g. Sleep disturbances, gastrointestinal disturbances, dizziness or disturbed sense of balance). A rare but important adverse reaction is acute brain syndrome which occurs in one in 5,000-20,000 of those taking the drug. It is not recommended for aircraft pilots or drivers of public transport.
MalaroneTM.
This is a combination of atovaquone and proguanil and recent studies have found it a safe and effective prophylactic agent with few side-effects. Unfortunately it is expensive ( US$42 for 12 tablets) and has to be taken daily. It is not suitable for those sensitive to atovaquone or proguanil. Treatment should be started 2 days before travel and continued for at least 7 days after a period of potential exposure to malaria.
Other possible regimens include daily azithromycin, daily high-dose primaquine and short course tafenoquine. It is emphasised that visitors to large towns or cities are much less at risk of catching malaria than travellers to rural areas. Bedrooms in multi-storey air-conditioned hotels are usually free of mosquitos. If living "rough" always sleep under a mosquito net. Make sure that it is free of holes, is well tucked in and ideally impregnated with Permethrin*. Alternatively, one of several new and more effective, recently introduced synthetic pyrethroids (e.g. deltamethrin), may be used which has been shown to be effective even after 20 washings of the impregnated net. Impregnation of the mosquito nets can be done at home prior to travelling. For adults travelling in rural or country areas where drug resistant P. falciparum malaria has been reported and where medical attention may not be available, standby treatment can be used as an alternative to, or in addition to, chemoprophylaxis. Potential standby drug regimes are those listed for the treatment of uncomplicated falciparum malaria (see treatment section) and include artemisinin-based regimens that can be purchased ‘over the counter' in many tropical countries.
There are now test kits for malaria* designed for those travelling in remote areas. These antigen detection kits allow a diagnosis of falciparum malaria (and other species in some cases) to be made quickly without other equipment and treatment can be started without delay. Self-diagnosis with a rapid test kit is not a substitute for a medical consultation but it could be useful in an emergency. With some kits, species-specific diagnoses are possible but all allow the identification of P. falciparum with reasonable accuracy. A multi-species, multi-strain vaccine has long been sought. By its very nature this is a complex and lengthy endeavour. Although vaccines have been produced, clinical trial results to date have been disappointing and it seems likely that a vaccine is still some time away. With the increasing spread and intensity of malarial resistance to drugs worldwide, prophylaxis can never be considered completely reliable and malaria must always be considered in febrile patients who have travelled to areas where malaria is endemic irrespective of whether chemoprophylactic agents have been used. It should be remembered that P. falciparum can sometimes cause sickness and death in a matter of hours and it is important to get to a medical practitioner FAST if you have fever and/or are disorientated. Test kits and emergency treatments are useful but are only aids.
* These items should be available from the Health Travel Medical Centre in
your State.
Treatment
P.falciparum
This species was originally sensitive to chloroquine. However, strains resistant
to this and other antimalarial drugs are now commonplace. Because the
parasite is able to multiply very rapidly and sequester within the
microvasculature, a life threatening illness may develop in a very short space of
time.
Uncomplicated malaria
Uncomplicated malaria is where patients can take oral therapy and can usually
be treated effectively with one of three regimens:
Quinine sulphate 10 mg salt/kg 8 hourly for seven days plus doxycycline 100 mg daily for 7 days. Patients will usually develop ‘cinchonism' (tinnitus, high-tone hearing loss, nausea, dysphoria) after 2-3 days but should be encouraged to complete the full course to avoid recrudescence. Tetracycline (4mg/kg daily for seven days) or the combination drug FansidarTM (25mg/kg sulfadoxine plus 1.25mg/kg pyrimethamine as a single dose) can be given as less expensive alternatives to doxycycline.
MalaroneTM (atovaquone 250 mg plus proguanil 100 mg) 4 tablets daily for three consecutive days. This combination therapy is relatively new and appears to be very effective but it is also very expensive. Resistance to this drug combination has already been reported in a patient from Nigeria (Malaria J. 2002; 1:1).
Mefloquine (LariumTM) given as 15 mg/kg in a divided dose followed by 10 mg/kg the following day. Antipyretic and antiemetic agents may need to be given prior to mefloquine administration to reduce the risk of vomiting.
With the advent of widespread chloroquine resistance, this drug (dose 25mg base/kg in divided doses over 2-3 days; see P. vivax treatment regimen below) can be combined with others such as FansidarTM (25mg/kg sulfadoxine plus 1.25mg/kg pyrimethamine as a single dose) in areas where background immunity to malaria contributes to parasite clearance and alternative regimens are too expensive. Lapdap (chlorproguanil 2mg/kg plus dapsone 2.5mg/kg) daily for three days is an inexpensive combination of well-established compounds being assessed in African trials.
Choice of regimen is based on:
Local cost and availability of antimalarial drugs
Area of malaria acquisition (i.e. drug resistance pattern of P. falciparum)
Prior chemoprophylaxis
Concomitant illnesses other than malaria
Age and pregnancy
Likely patient compliance with therapy
Risk of re-exposure to malaria after treatment
In uncomplicated cases in which nausea and vomiting preclude oral therapy, quinine dihydrochloride 10 mg salt/kg base can be given i.v. in 5% w/v dextrose or normal saline as a 4-hour infusion 8-hourly until the patient can take medication by mouth.
Severe malaria
Severe malaria is where patients have coma, jaundice, renal failure,
hypoglycaemia, lactic acidosis, severe anaemia, high parasite count,
hyperpyrexia. It is ideally treated in an intensive care or high dependency unit
where patients can be monitored closely both clinically and biochemically.
Intravenous quinine is the treatment of choice but rapid injection can lead to
hypotension, dysrhythmias and death.
In patients who have not received quinine in the previous 48 hours, one of two
regimens can be used:
Quinine dihydrochloride 20 mg salt/kg base given i.v. in 5% w/v dextrose or normal saline as a once-only 4 hour infusion followed, 4 hours later, by quinine dihydrochloride 10 mg salt/kg base 4-hour infusions, 8 hourly.
Where a syringe pump or other accurate infusion device is available, quinine dihydrochloride 7 mg salt/kg base over 30 minutes followed immediately by quinine dihydrochloride 10 mg salt/kg base over 4 hours then, starting 4 hours later, quinine dihydrochloride 10 mg salt/kg base as 4 hour infusions, 8 hourly.
Electrocardiographic monitoring can be done if available but is not essential unless additional cardiac risks are present. Where patients have received quinine within the previous 24 hours, give quinine dihydrochloride 10 mg salt/kg base i.v. in 5% w/v dextrose or normal saline as 4-hour infusions 8-hourly. Hypoglycaemia may occur in patients with severe malaria, particularly in those treated with quinine, and careful monitoring is required. Steroids should not be used in patients with severe malaria.
P.vivax
Most strains of P. vivax are still sensitive to chloroquine, although some
chloroquine resistant strains have been reported in Papua New Guinea,
Indonesia, Thailand and India. This drug will clear the erythrocyte stages of the
parasite but it has no effect on the exo-erythrocytic liver stage and a course of
primaquine (an 8-amino-quinoline) is required for radical cure. The Chesson
strain of P. vivax found in New Guinea shows some resistance to primaquine
and an increased dose is required but may still not result in radical cure. If
primaquine is not given, the patient may suffer a relapse which will occur
weeks, months or sometimes years after the original attack.
Adult treatment
(Based on Chloroquine tablets containing 150mg base)
4 tablets (600mg base) or 10 mg/kg first dose
2 tablets (300mg base) or 5 mg/kg 6-8 hours later
2 tablets (300mg base) or 5 mg/kg
2 tablets (300mg base) or 5 mg/kg
Next 14 days
primaquine 2 tablets (each tablet contains 7.5mg base daily with food)
The primaquine is preferably started after the chloroquine, at a dose of 3.5mg/kg given as a divided daily dose over 14 days. When the infection is acquired in New Guinea, up to 6mg/primaquine may be necessary (0.43mg/kg/day) should be given over 14 days. In the case of a relapse, repeat both chloroquine and primaquine treatment. Several relapses may occur before the parasite is finally eliminated. Unfortunately there is no other effective treatment. Tafenoquine is a newly developed long-acting, potent primaquine-like drug which may be available soon for radical cure. It can be given over 3 days instead of 14 but may not offer any advantage in efficacy over primaquine. Patients should have their G6PD status checked before primaquine (or tafenoquine) is prescribed. Those with G6PD deficiency may experience haemolysis if given a daily dose of primaquine and it is recommended that these patients be given 30-45mg once a week for 8 weeks. MalaroneTM may also be used to treat P. vivax malaria but a course of primaquine will still be required to eliminate liver forms.
P. malariae, P. ovale
Treatment for the eradication of these two strains of malaria is the same as that
for P. vivax except it is not necessary to give primaquine to those patients with
P. malariae.
Artemisinins
Artemisinin has been used for many years by the Chinese as a traditional
treatment for fever and malaria. It is a sesquiterpene lactone derived from the
wormwood plant Artemisia annua. Semi-synthetic derivatives including
artemether and artesunate are now widely available in the tropics. These
compounds are being increasingly used in a number of countries and are both
cheap and effective. They are starting to be licensed in Western countries.
They are particularly valuable in the treatment of multidrug-resistant falciparum
malaria. Unless used with a second antimalarial as described below there is
likely to be a high recrudescent rate. Side-effects have been reported but these
are comparartively rare and seldom severe. Artemisinin derivatives are
recommended for treatment but not for prophylaxis. If an artemisinin drug is
used to treat vivax malaria, it should be accompanied by a course of
primaquine.
Artemisinin (500mg tablets) give 10-20 mg/kg on day 1 (500-1,000 mg) orally then 500mg for 4 days. Then give mefloquine 15mg base/kg or split dose 25mg base/kg.
Artemisinin (200mg suppositories): for severe malaria 600-1200mg stat,
400-600mg after 4 hours then 400-800mg twice daily for 3 days. Give
mefloquine as above.
Artesunate (50 & 60 mg vials for intravenous use): for severe malaria
120mg I.V. stat. 60 mg at 4, 24 and 48 hours, 50-60 mg on days 3-5. Give
mefloquine as above.
Dihydroartemisinin (20 mg tablets): First dose 120mg then 60mg daily for 4-6 days then give mefloquine as above.
Artemeter (vials for intramuscular use): For severe malaria 3.2 mg/kg
intramuscularly stat then 1.6mg twice daily for 3-7 days. Give mefloquine
as above.
Caution:
A recent report on the sale of artesunate in South East Asia found that 38% of the artesunate purchased was fake (Lancet 2001; 357:1948-49). Fake artesunate can be identified by a dye test (J Pharm Biomed Anal 2000;24: 65-70). Other fake drugs including mefloquine can also be found in South East Asian markets.
Artemisinin-based combination therapies, some comprising a fixed co-formulation are being developed: Artesunate plus mefloquine is used in several Asian countries, some using blister packs to simplify dosing and increase compliance. The mefloquine component, which is usually given on the third day of artesunate treatment, is relatively expensive and side-effects are common. Artemether plus Iumefantrine (Co-artemTM or RiametTM) is an oral combination treatment but has problems with bioavailability of the fat-soluble lumefantrine component. Six doses have better efficacy than four, but cure rates have been variable. Dihydroartemisinin plus piperaquine (ArtekinTM, ArtecomTM, CV8, Duo-Cotexin) in a four-dose regimen has proved highly effective and well tolerated in South East Asian trials. Artesunate plus pyronaridine is under development in WHO-sponsored trials.
Source: http://www.rph.wa.gov.au/~/media/Files/Hospitals/RPH/PDFs/RoyalPerthHospital%20Malaria%20Resources.ashx
Internet Drug Outlet Identification Program Updated Progress Report for State and Federal Regulators: April 2012 – Re-Issued May 14, 2012 TABLE OF CONTENTS INTRODUCTION . 3 A. Findings of Site Reviews . 4 B. Recommended Internet Pharmacies . 5 C. Accreditation and Approval Applicant Screenings . 6 DRUG SHORTAGES CREATE NICHE FOR SWINDLERS . 6
Simplified access. Coordinated care. ProCeed Customer Solutions proCeed VIEKIRA HUB Referral Form PROVIDE SOLUTIONS TO Streamline access to VIEKIRA PAK for your patients using the enclosed proCeed Customer Solutions intake forms FINANCIAL ADHERENCE