Debeerdejager.co.za
Journal of the American College of Cardiology
Vol. 58, No. 8, 2011
2011 by the American College of Cardiology Foundation
ISSN 0735-1097/$36.00
Published by Elsevier Inc.
Age- and Sex-Related Differences inAll-Cause Mortality Risk Based on CoronaryComputed Tomography Angiography Findings
Results From the International MulticenterCONFIRM (Coronary CT Angiography Evaluation forClinical Outcomes: An International Multicenter Registry)of 23,854 Patients Without Known Coronary Artery Disease
James K. Min, MD,* Allison Dunning, MS,‡ Fay Y. Lin, MD,† Stephan Achenbach, MD,§Mouaz Al-Mallah, MD,储 Matthew J. Budoff, MD,¶ Filippo Cademartiri, MD,#Tracy Q. Callister, MD,** Hyuk-Jae Chang, MD,†† Victor Cheng, MD,‡‡ Kavitha Chinnaiyan, MD,§§Benjamin J. W. Chow, MD,储储 Augustin Delago, MD,¶¶ Martin Hadamitzky, MD,##Joerg Hausleiter, MD,## Philipp Kaufmann, MD,*** Erica Maffei, MS,# Gilbert Raff, MD,§§Leslee J. Shaw, PHD,††† Todd Villines, MD,‡‡‡ Daniel S. Berman, MD,‡‡ for theCONFIRM Investigators
New York and Albany, New York; Erlangen and Munich, Germany; Detroit and Royal Oaks, Michigan;Los Angeles, California; Parma, Italy; Hendersonville, Tennessee; Seoul, Korea; Ottawa, Ontario, Canada;Zurich, Switzerland; Atlanta, Georgia; and Washington, DC
We examined mortality in relation to coronary artery disease (CAD) as assessed by ⱖ64-detector row coronarycomputed tomography angiography (CCTA).
Although CCTA has demonstrated high diagnostic performance for detection and exclusion of obstructive CAD,
the prognostic findings of CAD by CCTA have not, to date, been examined for age- and sex-specific outcomes.
We evaluated a consecutive cohort of 24,775 patients undergoing ⱖ64-detector row CCTA between 2005 and2009 without known CAD who met inclusion criteria. In these patients, CAD by CCTA was defined as none (0%
stenosis), mild (1% to 49% stenosis), moderate (50% to 69% stenosis), or severe (ⱖ70% stenosis). CAD severitywas judged on a per-patient, per-vessel, and per-segment basis. Time to mortality was estimated using multivari-
able Cox proportional hazards models.
At a 2.3 ⫾ 1.1-year follow-up, 404 deaths had occurred. In risk-adjusted analysis, both per-patient obstructive(hazard ratio [HR]: 2.60; 95% confidence interval [CI]: 1.94 to 3.49; p ⬍ 0.0001) and nonobstructive (HR: 1.60;95% CI: 1.18 to 2.16; p ⫽ 0.002) CAD conferred increased risk of mortality compared with patients without evi-dent CAD. Incident mortality was associated with a dose-response relationship to the number of coronary ves-
sels exhibiting obstructive CAD, with increasing risk observed for nonobstructive (HR: 1.62; 95% CI: 1.20 to 2.19;
p ⫽ 0.002), obstructive 1-vessel (HR: 2.00; 95% CI: 1.43 to 2.82; p ⬍ 0.0001), 2-vessel (HR: 2.92; 95% CI: 2.00to 4.25; p ⬍ 0.0001), or 3-vessel or left main (HR: 3.70; 95% CI: 2.58 to 5.29; p ⬍ 0.0001) CAD. Importantly,the absence of CAD by CCTA was associated with a low rate of incident death (annualized death rate: 0.28%).
When stratified by age ⬍65 years versus ⱖ65 years, younger patients experienced higher hazards for death for2-vessel (HR: 4.00; 95% CI: 2.16 to 7.40; p ⬍ 0.0001 vs. HR: 2.46; 95% CI: 1.51 to 4.02; p ⫽ 0.0003) and3-vessel (HR: 6.19; 95% CI: 3.43 to 11.2; p ⬍ 0.0001 vs. HR: 3.10; 95% CI: 1.95 to 4.92; p ⬍ 0.0001) CAD. Therelative hazard for 3-vessel CAD (HR: 4.21; 95% CI: 2.47 to 7.18; p ⬍ 0.0001 vs. HR: 3.27; 95% CI: 1.96 to5.45; p ⬍ 0.0001) was higher for women as compared with men.
Among individuals without known CAD, nonobstructive and obstructive CAD by CCTA are associated with higher
rates of mortality, with risk profiles differing for age and sex. Importantly, absence of CAD is associated with a
very favorable prognosis.
(J Am Coll Cardiol 2011;58:849–60) 2011 by the American College of Cardiology
JACC Vol. 58, No. 8, 2011
Age- and Sex-Related Prognosis by CCTA
August 16, 2011:849 – 60
Coronary computed tomography
and Vascular Institute, Hendersonville, Tennessee; Capital
angiography (CCTA) is a re-
Cardiology Associates, Albany, New York; University of
cently introduced noninvasive
Munich, Munich, Germany; Ottawa Heart Institute, On-
CAD ⴝ coronary artery
imaging modality that permits
tario, Canada; Henry Ford Medical Center, Detroit, Mich-
accurate detection and exclusion
igan; Yonsei Medical Center, Seoul, Korea, University
CCTA ⴝ coronarycomputed tomography
of coronary artery disease (CAD)
Hospital, Zurich, Switzerland; William Beaumont Hospi-
Prior studies have exam-
tal, Royal Oak, Michigan; Walter Reed Army Medical
CI ⴝ confidence interval
ined the prognostic significance
Center, Washington, DC; and University Hospital of
of CAD detection by CCTA,
Parma, Parma, Italy). Institutional review board approval
but have been generally limited
was obtained at each center. Individuals with known CAD,
D-F ⴝ Diamond-Forrester
to single centers and small co-
as defined by prior myocardial infarction or coronary revas-
horts Given the enor-
cularization, were excluded from the present study analysis.
HR ⴝ hazard ratio
mous evidence base on prognosis
All patients were in normal sinus rhythm and were
LAD ⴝ left anteriordescending artery
with other cardiac imaging mo-
capable of the breath hold needed for CCTA. Patients with
dalities, the development of "real
⬎70 beats/min were given oral or intravenous
ⴝ left circumflex
world" effectiveness data that are
metoprolol as per local site protocol. All centers used
acquired across diverse health-
intravenous metoprolol at the time of CCTA performance
ⴝ left main artery
care settings and populations is a
to lower heart rates below 70 beats/min. If the patient's
RCA ⴝ right coronaryartery
requisite criterion to guide ap-
heart rate did not drop below 70 beats/min, then CCTA
propriate application of CCTA.
was performed at the lowest heart rate.
Fundamental to the use of
Before the initiation of the scan, we prospectively col-
lected information on the presence of categorical cardiac risk
factors in each individual. Systemic arterial hypertensionwas defined as a documented history of high blood pressure
CCTA is its ability to risk stratify younger and older women
or treatment with antihypertensive medications. Diabetes
and men. To date, however, age- and sex-specific outcomes
mellitus was defined by diagnosis of diabetes made previ-
of CCTA-identified CAD have been absent or exploratory
ously by a physician and/or use of insulin or oral hypogly-
To that end, we examined the predictive value of
cemic agents. Dyslipidemia was defined as known but
nonobstructive and obstructive CAD from a large cohort of
untreated dyslipidemia or current treatment with lipid-
23,854 patients without known CAD for intermediate-term
lowering medications. A positive smoking history was
mortality risk and further investigated the relationship of
defined as current smoking or cessation of smoking within
mortality risk to CAD as stratified by age and sex.
3 months of testing. Family history of coronary heart diseasewas determined by patient query. Symptom presentation
was classified into 1 of 4 categories: typical chest pain,
Patients. CONFIRM (Coronary CT Angiography Evalu-
atypical chest pain, noncardiac pain, or dyspnea
ation for Clinical Outcomes: An International Multicenter
Scan protocol and image reconstruction. The CCTA
Registry) enrolled consecutive adults ⱖ18 years of age
scans were performed on a variety of different scanner
between 2005 and 2009 who underwent ⱖ64-detector row
platforms (Lightspeed VCT, GE Healthcare, Milwaukee,
CCTA for suspected CAD at 12 centers (Cedars Sinai
Wisconsin; Somatom Definition CT, Siemens, Erlangen,
Medical Center, Los Angeles, California; Harbor UCLA
Germany; Somatom Definition Flash CT, Siemens). Im-
Medical Center, Los Angeles, California; Tennessee Heart
Dr. Min received modest speakers' bureau and medical advisory board compensation and
From the *Department of Medicine, Cedars-Sinai Heart Institute, Cedars-Sinai
significant research support from GE Healthcare. Dr. Achenbach received grant support
Medical Center, Los Angeles, California; †Department of Medicine, Weill Cornell
from Siemens and Bayer Schering Pharma and has served as a consultant for Servier. Dr.
Medical College and the New York Presbyterian Hospital, New York, New York;
Al-Mallah received support from the American Heart Association, BCBS Foundation of
‡Department of Public Health, Weill Cornell Medical College and the New York
Michigan, and Astellas. Dr. Budoff received modest speakers' bureau compensation from
Presbyterian Hospital, New York, New York; §Department of Medicine, University
GE Healthcare. Dr. Cademartiri received grant support from GE Healthcare. Dr.
of Erlangen, Erlangen, Germany; 储Department of Medicine, Wayne State University,
Callister has served on the Speakers' Bureau of General Electric Healthcare. Dr.
Henry Ford Hospital, Detroit, Michigan; ¶Department of Medicine, Harbor UCLA
Chinnaiyan received grant support from Bayer Pharma and Blue Cross Blue Shield Blue
Medical Center, Los Angeles, California; #University Hospital of Parma, Parma,
Care MI. Dr. Chow received research and fellowship support from GE Healthcare,
Italy; **Tennessee Heart and Vascular Institute, Hendersonville, Tennessee; ††Divi-
research support from Pfizer and AstraZeneca, and educational support from TeraRecon.
sion of Cardiology, Severance Cardiovascular Hospital, Seoul, Korea; ‡‡Department
Dr. Hausleiter received a research grant from Siemens Medical Systems. Dr. Kaufmann
of Imaging, Cedars Sinai Medical Center, Los Angeles, California; §§William
received institutional research support from GE Healthcare and grant support from Swiss
Beaumont Hospital, Royal Oaks, Michigan; 储 储Department of Medicine and Radi-
National Science Foundation. Dr. Maf ei has served as a consultant to Servier and has
ology, University of Ottawa, Ontario, Canada; ¶¶Capitol Cardiology Associates,
received grant support from GE Healthcare. Dr. Raff received grant support from Siemens,
Albany, New York; ##Division of Cardiology, Deutsches Herzzentrum Munchen,
Blue Cross Blue Shield Blue Care MI, and Bayer Pharma. All other authors have reported that
Munich, Germany; ***University Hospital, Zurich, Switzerland; †††Department of
they have no relationships relevant to the contents of this paper to disclose.
Medicine, Emory University School of Medicine, Atlanta, Georgia; and the ‡‡‡Depart-
Manuscript received December 19, 2010; revised manuscript received February 16,
ment of Medicine, Walter Reed Medical Center, Washington, DC.
2011, accepted February 22, 2011.
JACC Vol. 58, No. 8, 2011
August 16, 2011:849 – 60
Age- and Sex-Related Prognosis by CCTA
aging of a test bolus of contrast was performed at 2 mm
was highly calcified, 2-dimensional oblique images were also
superior to the take-off of the left main coronary artery for
visualized without maximal-intensity projection (i.e., 0.625-
precise timing of contrast injection. During the CCTA
to 0.75-mm isotropic voxel resolution) or multiplanar re-
acquisition, 80 to 140 ml of iodinated contrast (Isovue 370,
formats with cross-sectional views to minimize partial-
Bracco Diagnostics, Princeton, New Jersey; Omnipaque,
volume averaging artifact of calcium.
GE Healthcare, Princeton, New Jersey; Visipaque, GE
Plaque severity was graded on a per-patient, per-vessel,
Healthcare, Princeton, New Jersey; or Imeron 350; Bracco
and per-segment level. Per-patient maximal plaque severity
Atlana Pharma, Konstanz, Germany) was injected, followed
was defined by the maximal intraluminal stenosis in any of
by a 50-ml saline flush. Contrast timing was performed to
the coronary segments at the ⱖ50% stenosis or ⱖ70%
optimize uniform contrast enhancement of the coronary
stenosis threshold.
arteries. The scan parameters were as follows: 64 ⫻ 0.625/
For purposes of classification for per-vessel analyses, we
0.750-mm collimation, tube voltage 100 or 120 mV, effec-
considered 4 arterial territories: left main artery (LM), left
tive 400 to 650 mA. Dose reduction strategies—including
anterior descending artery (LAD), left circumflex artery
electrocardiogram-gated tube current modulation, reduced
(LCx), and right coronary artery (RCA). Obstructive CAD
tube voltage, and prospective axial triggering—were used
in the diagonal branches, obtuse marginal branches, and
whenever feasible. Estimated radiation dose for CCTA
posterolateral branches was considered as part of the LAD,
ranged from 3 to 18 mSv.
LCx, and RCA system, respectively. The posterior descend-
Helical or axial scan data were obtained with retrospective
ing artery was considered as part of the RCA or LCx
or prospective electrocardiogram gating, respectively. Im-
system, depending on the coronary artery dominance. A
ages were reconstructed immediately after completion of the
ⱖ50% stenosis in the LM was considered obstructive in all
scan to identify motion-free coronary artery images. Opti-
models. Per-vessel CAD severity was defined by ⱖ50%
mal phase reconstruction was assessed by comparison of
stenosis or ⱖ70% stenosis in 0, 1, 2, or 3 coronary artery
different phases, if available, and the phase with the least
amount of coronary artery motion was chosen for analysis.
Per-segment analysis was judged for individual coro-
Multiple phases were utilized for image interpretation if
nary artery segments that included a 16-segment model,
minimal coronary artery motion was different for different
as we have previously described Similarly, the incre-
arteries. CCTAs were evaluated by an array of post-
mental hazards of CAD for increasing numbers of
processing imaging techniques, including axial, multiplanar
segments were calculated as clinical coronary artery
reformat, maximum-intensity projection, and short-axis
plaque scores, as we have previously described A
cross-sectional views. In all individuals, irrespective of
segment involvement score was calculated as the total
image quality, every arterial segment was scored in an
number of coronary artery segments exhibiting plaque,
intent-to-diagnose fashion. If a coronary artery segment was
irrespective of the degree of luminal stenosis within each
uninterpretable despite these multiple techniques, the non-
segment (minimum ⫽ 0; maximum ⫽ 16). A segment
evaluable segment was scored similarly to the most proximal
stenosis score was used as a measure of overall coronary
segment that was evaluable.
artery plaque extent. Each individual coronary segment
Noninvasive coronary artery analysis by CCTA. All
was graded as having no to severe plaque (i.e., scores from
scans were analyzed by Level III– equivalent cardiologists
0 to 3) based on extent of obstruction of coronary luminal
with experience interpreting several thousand CCTA scans.
diameter. Then the extent scores of all 16 individual
Interpretation of CCTA was uniform across all study sites,
segments were summed to yield a total score ranging
with coronary segments visually scored for the presence of
from 0 to 48. We further examined risk in association
coronary plaque using a 16-segment coronary artery model
with any severe proximal stenosis in the LAD, LCx, or
in an intent-to-diagnose fashion. In each coronary artery
RCA vessels. Finally, we examined risk for any plaque
segment, coronary atherosclerosis was defined as tissue
within the LM.
structures ⬎1 mm2 that existed either within the coronary
Follow-up. The primary endpoint was time to death from
artery lumen or adjacent to the coronary artery lumen that
all causes. Follow-up procedures were approved by all study
could be discriminated from surrounding pericardial tissue,
centers' institutional review boards. Death status for non-
epicardial fat, or the vessel lumen itself. Coronary athero-
U.S. centers was gathered by clinical visits, telephone
sclerotic lesions were quantified for stenosis by visual esti-
contacts, and questionnaires sent by mail, with verification
mation. Luminal-diameter stenosis severity was scored as
of all reported events by hospital records or direct contact
none (0% luminal stenosis), mild (1% to 49% luminal
with a patient's attending physician. Death status for U.S.
stenosis), moderate (50% to 69% luminal stenosis), or severe
centers was ascertained either by query of the Social Security
(ⱖ70% luminal stenosis). Percent obstruction of coronary
Death Index or by scripted interview by experienced physi-
artery lumen was based on a comparison of the luminal
cian and/or nurse study investigators.
diameter of the segment exhibiting obstruction to the
Statistical analysis. SPSS version 12.0 (SPSS Inc., Chi-
luminal diameter of the most normal-appearing site imme-
cago, Illinois) and SAS version 9.2 (SAS Institute, Cary,
diately proximal to the plaque. In instances in which plaque
North Carolina) were used for all statistical analyses.
JACC Vol. 58, No. 8, 2011
Age- and Sex-Related Prognosis by CCTA
August 16, 2011:849 – 60
Demographics of the Entire Registry and Study Cohort
Demographics of the Entire Registry and Study Cohort
Excluded Patients
Family history of premature CAD
History of PAD/CVD
Pre-test CAD likelihood†
Values are mean ⫾ SD or n (%). *p value for differences in percentages for study cohort versus excluded patients. †Typicality of chest pain andpre-test likelihood of CAD missing in 518 patients.
CAD ⫽ coronary artery disease; CVD ⫽ cardiovascular disease; PAD ⫽ peripheral arterial disease.
Categorical variables are presented as frequencies and
ratio (HR) and 95% confidence interval (CI) were calcu-
continuous variables as mean ⫾ SD. Variables were
lated from the Cox models. A 2-tailed p ⬍ 0.05 was
compared with chi-square statistic for categorical vari-
considered statistically significant.
ables and by Student unpaired
t test for continuousvariables. Time to death from all causes and death rates
were calculated using univariable Cox proportional haz-ards models. In each case, the proportional hazards
Clinical characteristics of the study cohort. Amongst
assumption was met. Adjusted models were also devised
27,125 consecutive patients undergoing CCTA at 12 cen-
including multivariable stepwise models adjusting for
ters for whom per-segment CAD data were available, 2,350
baseline demographics, cardiac risk factors, typicality of
patients with a history of myocardial infarction, coronary
angina, and pre-test likelihood of obstructive CAD.
revascularization, and cardiac transplant were excluded. The
Adjusted models were also developed to test first-order
final analysis cohort consisted of 24,775 patients. Follow-up
interactions related to age, sex, and study site. A hazard
was obtained for 23,854 patients (96.3%), with 921 patients
Clinical Characteristics of Study Group Stratified by Normal, Nonobstructive, and Obstructive CAD by CCTA
Clinical Characteristics of Study Group Stratified by Normal, Nonobstructive, and Obstructive CAD by CCTA
Nonobstructive CAD
p Value for Trend
Family history of premature CAD
Chest pain typicality*
Pre-test CAD likelihood
Values are n (%). *Chest pain typicality and pre-test likelihood of CAD missing in 2,867 patients.
CAD ⫽ coronary artery disease; CCTA ⫽ coronary computed tomography angiography.
JACC Vol. 58, No. 8, 2011
August 16, 2011:849 – 60
Age- and Sex-Related Prognosis by CCTA
CCTA findings among those who lived versus died. As
Clinical Characteristics Associated With Mortality
Clinical Characteristics Associated With Mortality
compared with patients who were alive at follow-up, pa-
Univariate HR (95% CI)
tients who died had significantly more severe coronary artery
1.09 (1.08–1.10)
stenoses in the majority of coronary segments
1.05 (0.87–1.28)
Impact of per-patient, per-vessel, and per-segment CAD
2.13 (1.71–2.65)
severity by CCTA on death from all causes. In both
1.93 (1.57–2.37)
univariable as well as multivariable Cox regression anal-
0.71 (0.59–0.87)
ysis considering age and CAD risk factors, all-cause
1.47 (1.17–1.85)
mortality was predicted by maximal per-patient nonob-
Family history of premature CAD
1.11 (0.90–1.36)
Pre-test CAD likelihood
1.20 (0.996–1.45)
structive and obstructive CAD, whether using a defini-tion of obstructive CAD as 1% to 49% or 1% to 69%
CAD ⫽ coronary artery disease; CI ⫽ confidence interval; HR ⫽ hazard ratio.
By both univariable and multivariable Cox models, per-
lost to follow-up. The study cohort was middle-aged (age
vessel assessment of obstructive CAD demonstrated a dose-
57 ⫾ 13 years, 54% male) with a high prevalence of
response relationship for increased hazards for death for
cardiovascular risk factors and symptoms. They presentedwith typical or atypical angina in the majority of cases, with
1-vessel, 2-vessel, 3-vessel, or LM CAD
the majority of individuals having intermediate or high
Similarly, in both univariable and multivariable Cox regres-
pre-test likelihood of obstructive CAD. Excluded patients
sion analysis, on a per-segment basis, higher rates of
had a higher pre-test likelihood of CAD
mortality were associated with greater numbers of segments
Clinical characteristics associated with CAD and mortality.
with plaque, with stenosis-adjusted segments with plaque,
Survival was examined after a mean follow-up of 2.3 ⫾ 1.1
with any severe proximal stenosis, and with any plaque
years (median 2.1 years; interquartile range: 1.5 to 3.1
years), at which point 404 deaths were recorded. Increasing
Sixty-six deaths (0.65%) occurred in patients without
severity of CAD was associated with male sex, diabetes,
evident CAD by CCTA (n ⫽ 10,146; 43%), resulting in a
hypertension, dyslipidemia, family history of CAD, current
mean annualized death rate of 0.28%. In additional analyses
smoking, typical angina, and high pre-test likelihood of
of patients undergoing CCTA followed for ⱖ4 years (n ⫽
CAD (p ⬍ 0.0001 for all) In univariable Cox
1,816) without evidence by CCTA (n ⫽ 1,009), annualized
proportional hazards models, increased hazard for death was
death rates were 0.22%.
associated with advanced age, diabetes, hypertension, un-
Age- and sex-stratified impact of CCTA-visualized CAD
treated dyslipidemia, and current smoking, but not family
on death from all causes. Individuals ⬍65 years of age had
history of CAD or pre-test CAD likelihood
lower pre-test probability of CAD than those ⱖ65 years of
Coronary Artery Stenosis Severity by Segment For Individuals Who Lived Versus Died
Coronary Artery Stenosis Severity by Segment For Individuals Who Lived Versus Died
Alive (n ⴝ 23,450)
Diagonal artery 1
Diagonal artery 2
Obtuse marginal 1
Obtuse marginal 2
Right coronary artery
Posterior descending artery
CAD ⫽ coronary artery disease; LAD ⫽ left anterior descending artery; LCx ⫽ left circumflex artery; LM ⫽ left main artery; PL ⫽ posterolateral.
JACC Vol. 58, No. 8, 2011
Age- and Sex-Related Prognosis by CCTA
August 16, 2011:849 – 60
Per-Vessel, and Adjusted
Hazard Ratios Mortality
All-Cause Per-Patient,
Mortality by Stenosis Level
Per-Vessel, and Per-Segment Analysis by Obstructive CAD at the 50% and 70% Stenosis Level
Obstructive CAD (Defined at 50% Level)
Obstructive CAD (Defined at 70% Level)
Per-patient analysis
Nonobstructive CAD
2.88 (2.15–3.86)
1.60 (1.18–2.16)
3.29 (2.50–4.34)
1.76 (1.32–2.34)
6.05 (4.58–7.99)
2.60 (1.94–3.49)
8.11 (6.00–11.0)
3.13 (2.27–4.31)
Per-vessel analysis
2.88 (2.15–3.86)
1.62 (1.20–2.19)
3.30 (2.50–4.34)
1.77 (1.33–2.36)
1-vessel obstructive
4.12 (2.96–5.72)
2.00 (1.43–2.82)
5.67 (3.97–8.10)
2.35 (1.62–3.42)
2-vessel obstructive
6.93 (4.82–9.96)
2.92 (2.00–4.25)
11.40 (7.56–17.2)
3.94 (2.57–6.04)
3-vessel or left main
10.52 (7.50–14.7)
3.70 (2.58–5.29)
15.52 (10.1–23.9)
5.27 (3.36–8.27)
Per-segment analysis
Segment involvement score
1.22 (1.18–1.25)
1.10 (1.06–1.13)
(per segment involved)
Segment stenosis score (per
1.12 (1.11–1.14)
1.06 (1.05–1.08)
segment severity)
Any severe proximal stenosis
4.01 (3.12–5.17)
2.15 (1.66–2.78)
Any left main stenosis
2.51 (2.01–3.13)
1.45 (1.15–1.82)
NA ⫽ not applicable; other abbreviations as in
age (pre-test probability low 34% vs. 16%; intermediate 60%
hazards for mortality if 2- or 3-vessel/LM obstructive CAD
vs. 67%, high 6% vs. 17%, chi-square p ⬍ 0.0001). As
was present than patients ⱖ65 years of age, with similar
compared with individuals without CAD within respective
rates of death for nonobstructive and 1-vessel obstructive
age groups, patients ⬍65 years of age experienced higher
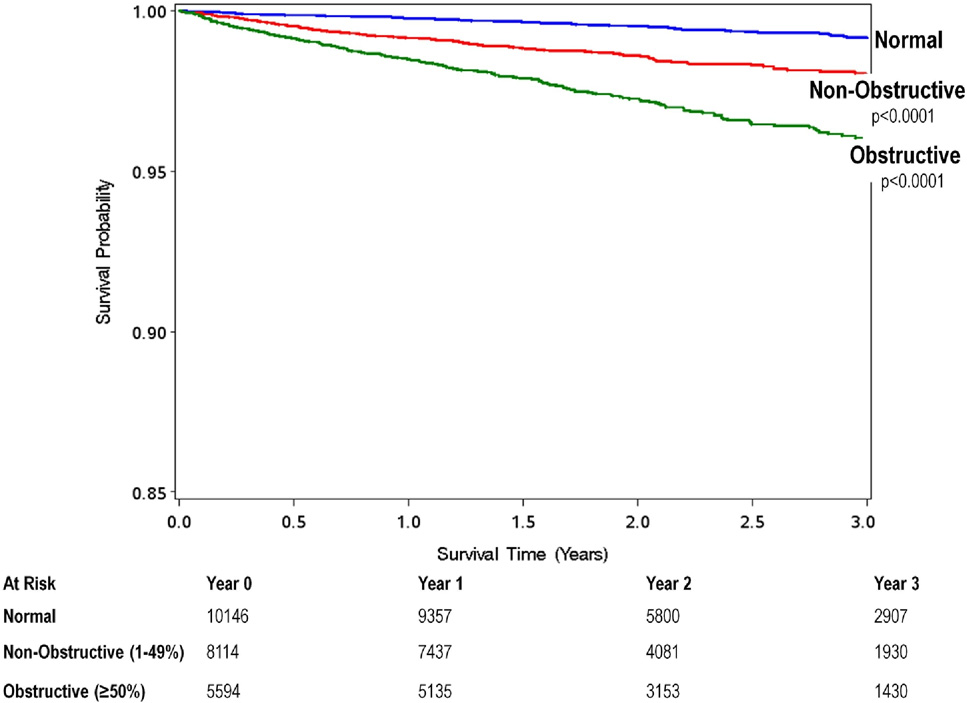
Unadjusted All-Cause 3-Year Kaplan-Meier Survival by the Maximal Per-Patient Presence
of None, Nonobstructive, and Obstructive CAD
Patients with nonobstructive coronary artery disease (CAD) had an intermediate prognosis that resides between patients with no evident CAD and those with obstructive CAD.
JACC Vol. 58, No. 8, 2011
August 16, 2011:849 – 60
Age- and Sex-Related Prognosis by CCTA
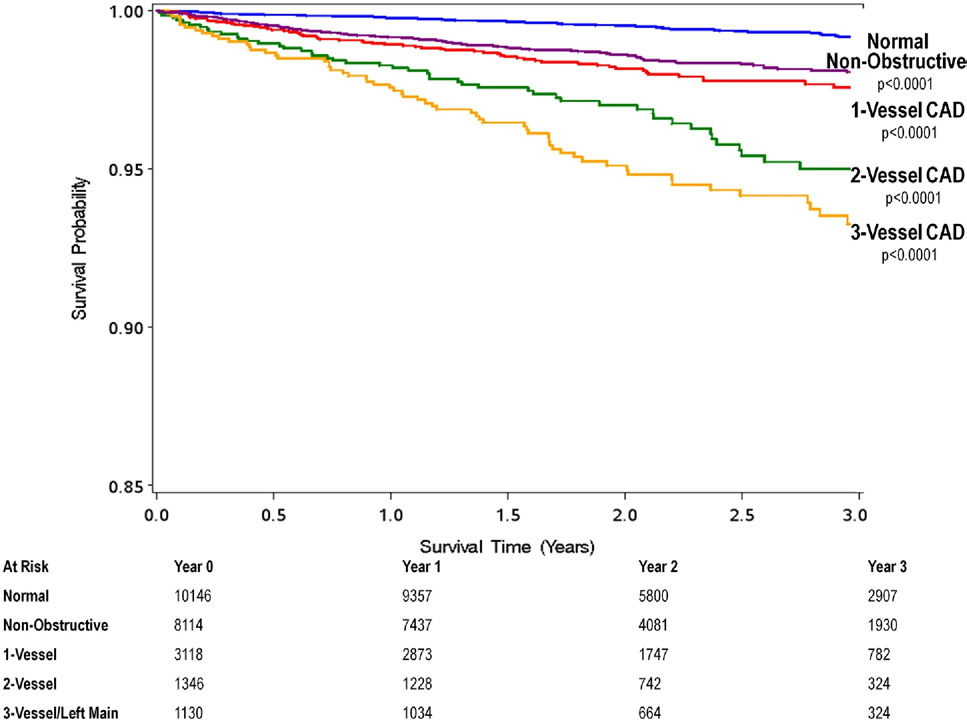
Unadjusted All-Cause 3-Year Kaplan-Meier Survival by the Presence, Extent, and Severity of CAD by CCTA
Note the dose-response relationship of mortality to increasing numbers of vessels with obstructive coronary artery disease (CAD).
CCTA ⫽ coronary computed tomography angiography.
Female patients referred to CCTA had higher pre-test
and CAD (p ⫽ 0.21) and sex and CAD (p ⫽ 0.76) did not
probability of CAD than men. Differences in pre-test
reveal significant relationships.
likelihood for obstructive CAD existed by sex, with maleand female patients presenting with low (pre-test probabil-
ity low 35% vs. 24%, intermediate 56% vs. 68%, and high9% vs. 9%; p ⬍ 0.0001). As compared with individuals
These results of the CONFIRM registry represent the first
without CAD within respective sexes, women experienced
prospective international multicenter data to relate CCTA-
higher hazards for mortality for 3-vessel or LM obstructive
determined extent and severity of CAD to all-cause mor-
CAD than males, with similar rates of death for nonob-
tality and demonstrate the independent prognostic value of
structive, 1-vessel, and 2-vessel obstructive CAD
both obstructive as well as nonobstructive CAD by CCTA.
Importantly, this study had adequate sample size and was
When stratified by both age and sex, differences in
adequately powered (beta ⬎0.90, alpha ⬍0.001) to permit
multivariable risk-adjusted hazards for mortality were ob-
differential risk stratification of individuals as categorized by
served for nonobstructive and 1-, 2-, and 3-vessel or LM
age group and sex. The findings of this study should be
obstructive CAD Tests for interactions of age
considered widely generalizable, given the high number of
Versus > All-Cause
All-Cause Mortality
for Patients <65 Versus >65 Years of Age
Age <65 Yrs
3-vessel disease or left main disease
Abbreviations as in
JACC Vol. 58, No. 8, 2011
Age- and Sex-Related Prognosis by CCTA
August 16, 2011:849 – 60
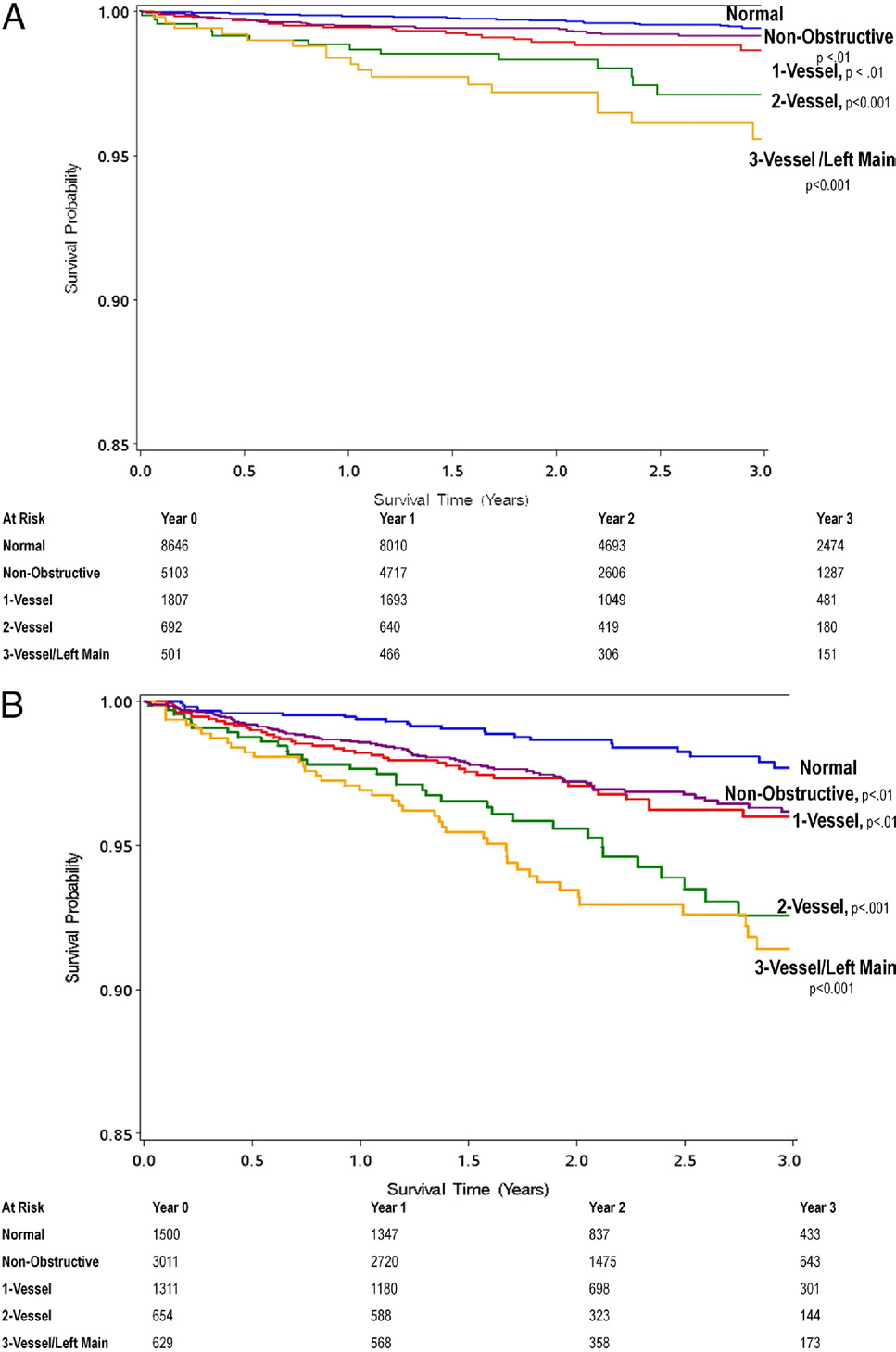
Unadjusted All-Cause 3-Year Kaplan-Meier Survival by Presence, Extent, and Severity of CAD
by CCTA as Stratified by Age <65 or >65 Years
Although rates of mortality in relationship to CAD extent are lower in patients age ⬍65 years (A), patients age ⬍65 years with 2- and 3-vessel CAD experience a higherrelative rate of mortality referenced to patients age ⬍65 years with no CAD in comparison with patients age ⱖ65 years with 2- and 3-vessel CAD referenced to patientsage ⱖ65 years with no CAD (B). Abbreviations as in
JACC Vol. 58, No. 8, 2011
August 16, 2011:849 – 60
Age- and Sex-Related Prognosis by CCTA
Adjusted Hazard Ratios for All-Cause Mortality for Female Versus Male Patients
Adjusted Hazard Ratios for All-Cause Mortality for Female Versus Male Patients
3-vessel/left main disease
Abbreviations as in
enrolled subjects; the inclusion of numerous clinical sites
assessment The current data suggest that use of the
within North America, Europe, and Asia; and the unifor-
D-F method is insufficient for this purpose and should not
mity of study results across sites.
be used solely as a judge of risk.
Despite increasing adoption of CCTA for clinical use in
We also identified a utility of nonobstructive CAD
individuals with suspected CAD, limited "real world" effec-
detection for risk stratification of individuals at height-
tiveness evidence still exists to support the prognostic
ened risk of incident death. Indeed, individuals with
significance of CAD findings as detected by current-
nonobstructive CAD (HR: 1.62; 95% CI: 1.08 to 2.43)
generation ⱖ64-detector row CCTA. Furthermore, prior
by CCTA experienced a mortality risk that was similar to
studies to date that have examined the ability of CCTA
that of those with obstructive 1-vessel CAD (HR: 1.75;
findings to stratify risk have been generally limited to single
95% CI: 1.12 to 2.72). These data corroborate our prior
centers with relatively small sample sizes. We previously
studies using older generation electron beam CT tech-
reported the predictive value of CCTA measures of CAD
nology, where the presence of nonobstructive CAD
extent and severity in a 2-center study of 5,330 consecutive
conferred similar risk as 1-vessel obstructive CAD. These
patients, but data were limited in that population to vessel-
findings have important implications, as patients with
based analyses, and the prognostic potential of segment-
nonobstructive CAD comprise the majority of patients
based as well as nonobstructive CAD detection by CCTA
who experience myocardial events and for whom func-
could not be examined In a separate analysis, we
tional stress testing aimed at detecting flow-limiting
reported the prognostic significance of CCTA-identified
coronary artery stenoses would be expectedly negative
CAD findings in 1,256 consecutive patients with suspected
Given a robust evidence base demonstrating the
CAD for the prediction of major adverse cardiac events
highly salutatory effect of primary prevention of CAD
Although we noted a 16- to 17-fold increased risk in
events in at-risk individuals, future studies should be
myocardial events in patients with obstructive CAD, the
performed to determine the effect of aggressive medical
observed event rates were low (0.6% to 1.8%) and the
therapy and lifestyle modification for individuals with
follow-up duration shorter than in the present study. In this
CCTA-identified nonobstructive CAD.
regard, the current data extend prior studies by examining
We recently reported the results of an exploratory
CCTA findings of CAD in a large consecutive cohort
analysis of 1,127 consecutive patients with suspected
comprising multiple international sites that was evaluated by
CAD undergoing 16-detector row CCTA identified to
current-generation computed tomography (CT) technology
have only obstructive CAD. In this study, 490 patients
for measures of both obstructive and nonobstructive CAD.
were identified as having nonobstructive CAD (as de-
That CCTA can effectively risk stratify individuals without
fined by maximal ⬍50% luminal diameter stenosis at the
known CAD should be invaluable for guiding the develop-
per-patient level) In 4-year follow-up, the number
ment of clinical practice guidelines and appropriate use
of coronary segments exhibiting nonobstructive CAD
was predictive of incident death in women but not in
One notable finding in our study was that although the
men. This study expands on these prior published results
pre-test likelihood of obstructive CAD—as estimated by
by using a study cohort of sufficient magnitude to
the Diamond-Forrester (D-F) tabular method—was highly
examine the presence of nonobstructive CAD at the
predictive of the presence of obstructive CAD by CCTA, it
per-patient level. The present data corroborate the prior
did not demonstrate predictive value for incident death in
data, revealing a prognostic value for per-patient nonob-
this large cohort of patients with suspected CAD. At
structive CAD detection in women but not in men.
present, clinicians commonly use D-F pre-test estimations
Further, the current study extends prior study results by
of likelihood of obstructive CAD as a metric to determine
demonstration that 1-vessel obstructive CAD also con-
whether patients would benefit from noninvasive testing.
fers heightened risk of death in women but not in men.
Because global clinical risk scores are currently lacking for
Numerous possibilities exist to explain these findings.
symptomatic stable individuals with suspected CAD, many
Women in our study had lower rates of both obstructive
have also adopted use of the D-F method for "risk"
and nonobstructive CAD in contrast to their male
JACC Vol. 58, No. 8, 2011
Age- and Sex-Related Prognosis by CCTA
August 16, 2011:849 – 60
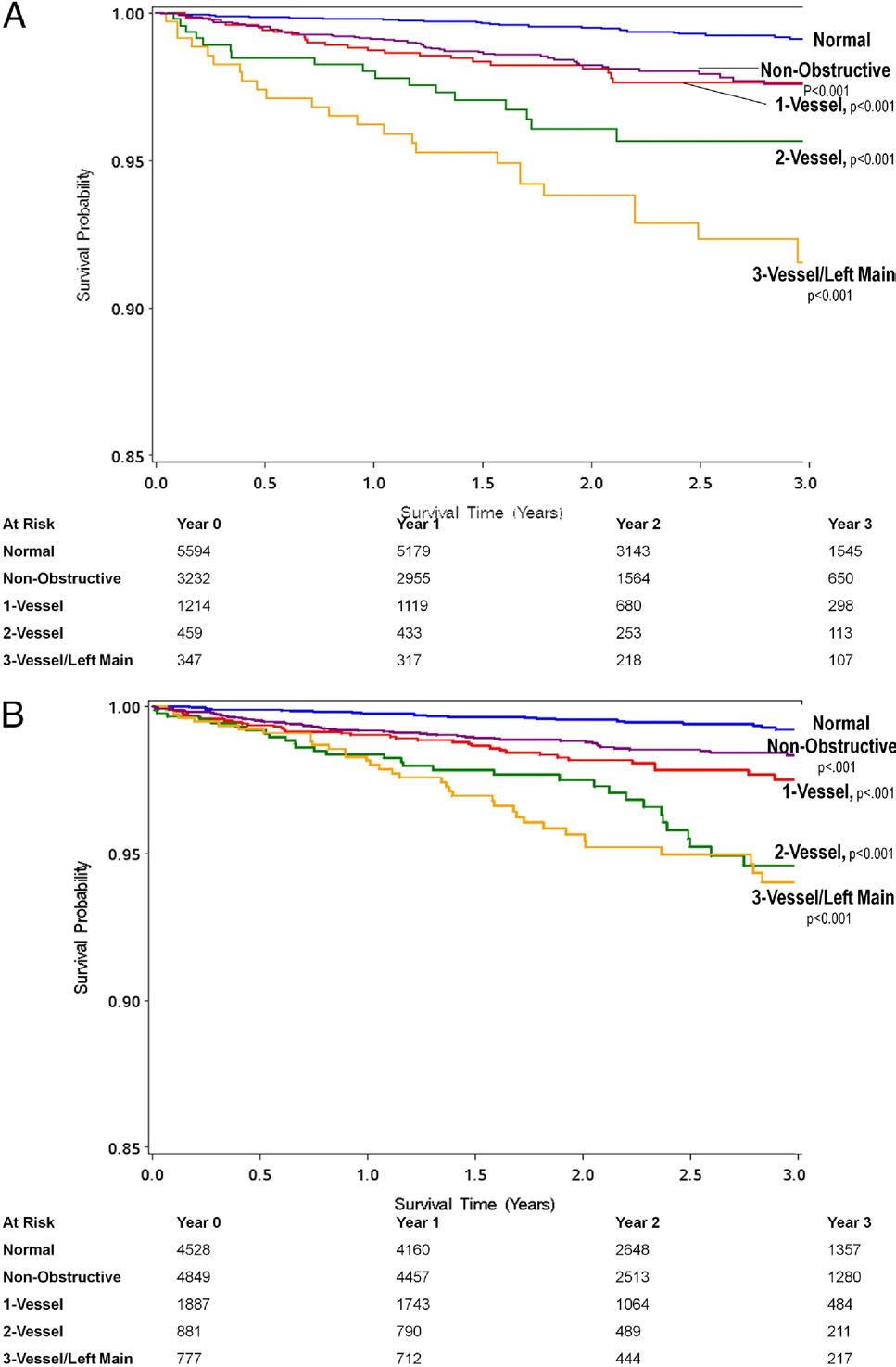
Unadjusted All-Cause 3-Year Kaplan-Meier Survival by Presence, Extent, and Severity of CAD by CCTA as Stratified by Sex
Although rates of mortality in relationship to CAD extent are lower in women, women with 3-vessel CAD experience a higher relative rate of mortality referenced to
women with no CAD (A) in comparison with men with 3-vessel CAD referenced to men with no CAD (B). Abbreviations as in
counterparts, despite higher estimated pre-test probabil-
to "exclusion" of cardiac causes of symptoms in women,
ity. This generally lower prevalence of disease in women
despite a higher rate of hospitalization for angina as
has been historically associated with lower rates of
compared with men It remains possible in this
invasive coronary angiographic evaluation and often leads
open-label study that the identification of nonobstructive
JACC Vol. 58, No. 8, 2011
August 16, 2011:849 – 60
Age- and Sex-Related Prognosis by CCTA
Multivariable Adjusted Hazard Ratios for All-Cause Mortality as Stratified by Age and Sex
Multivariable Adjusted Hazard Ratios for All-Cause Mortality as Stratified by Age and Sex
Age <65 Yrs
3-vessel/left main disease
Abbreviations as in
disease in women led clinicians to pursue alternative
future studies examining the risk of major adverse cardiac
noncardiac diagnoses for symptoms, and lack of aggressive
events in relation to CCTA findings. Further, referral bias due
treatment for these CAD findings resulted in heightened risk of
to excluded patients and treatment of individuals based on
incident death. Future studies should carefully evaluate this
CCTA findings of CAD are unknown in this open-label
potential explanation and should determine the effect of
multicenter registry. Whether percutaneous or surgical coro-
primary prevention with aggressive medical therapy in this
nary revascularization, enhanced medical therapy, or lifestyle
modifications occurred after CCTA performance is unknown.
In the present study, we also observed differential risk
We have previously demonstrated that CAD risk factor control
stratification of CCTA-identified CAD findings by age
is improved in direct relation to the extent and severity of
groups. Although risk of all-cause death increased in a
CCTA CAD findings, but whether this affects mortality has
generally linear fashion for patients ⱖ65 years of age for
not been explored. For proper evaluation of this issue, large-
extent and severity of CAD, patients ⬍65 years of age
scale trials with prescribed treatment algorithms will be neces-
experienced a more abrupt increase in risk of death associ-
sary. In addition, our analysis entailed the evaluation of CAD
ated with 2- and 3-vessel or LM CAD over nonobstructive
by semiquantitative visual analysis rather than by volumetric
or 1-vessel CAD. Although numerous explanations exist to
quantification of plaque. At the time of initiation of the study
account for these findings, it may be that younger patients
(and to date), no automated validated software existed for
with greater extent and severity of CAD represent a cohort
automatic quantification of plaque or stenosis severity. Instead,
with more aggressive forms of atherosclerosis than their
this multicenter study used experienced level III CCTA
older counterparts, thus resulting in a higher risk than for
imagers and used a uniform grading system that is most
older patients with more insidious atherosclerosis.
commonly used in daily clinical practice. Finally, this study
Finally, we observed a very low rate of death for individuals
examined only patients without history of known CAD. As
without evident CAD by CCTA. This low rate of death
such, whether these findings can be extrapolated to those with
validates the favorable prognosis that has been uniformly
prior myocardial infarction or coronary revascularization needs
observed in prior smaller registries and emphasizes a clinical
to be tested in future studies.
value of CCTA for identification of individuals in whom nofurther additional testing and/or therapy is necessary or indi-cated Using older generation electron beam CT
technology, Ostrom et al. demonstrated that this very lowdeath rate continues to persist for up to 7 years from the time
In the large, prospective, international, multicenter CONFIRM
of the CCTA, and the present results are in direct accordance
registry, extent and severity of CAD by CCTA successfully
with those findings. Similarly, the long-term ⱖ4-year progno-
identifies individuals at heightened risk for all-cause mor-
sis of patients in the present registry without evident CAD by
tality. Presence of both obstructive and nonobstructive
CCTA was extremely favorable, with a 0.22% annualized
CAD by CCTA on a per-patient, per-vessel, and per-
death rate. These results may inform clinicians on the need for
segment basis portends worsened prognosis, with differen-
repeat testing in patients with normal CCTA and suggest a
tial risk noted between sex and age groups. Importantly,
"warranty" period of a normal CCTA to last at least 4 years.
individuals without evident CAD by CCTA are at very low
Study limitations. Although this study addresses many of
risk of death.
the shortcomings of prior analyses examining the prognosticvalue of CCTA, it is not without limitations. For the present
Reprint requests and correspondence: Dr. James K. Min, De-
analysis, the major endpoint was all-cause mortality. Other
partments of Medicine, Imaging and Biomedical Sciences,
"softer" endpoints—including myocardial infarction, unstable
Cedars-Sinai Heart Institute, Cedars-Sinai Medical Center, 8700
angina, or CAD-related hospitalization—were not included in
Beverly Blvd, S. Taper Bldg, Room 1258, Los Angeles, CA
this initial analysis. Although use of all-cause death mitigates
ascertainment bias, it will nevertheless be important to perform
JACC Vol. 58, No. 8, 2011
Age- and Sex-Related Prognosis by CCTA
August 16, 2011:849 – 60
coronary atherosclerosis, and left ventricular ejection fraction. J AmColl Cardiol 2010;55:1017–28.
1. Budoff MJ, Dowe D, Jollis JG, et al. Diagnostic performance of
12. van Werkhoven JM, Schuijf JD, Gaemperli O, et al. Incremental
64-multidetector row coronary computed tomographic angiography
prognostic value of multi-slice computed tomography coronary an-
for evaluation of coronary artery stenosis in individuals without known
giography over coronary artery calcium scoring in patients with
coronary artery disease: results from the prospective multicenter
suspected coronary artery disease. Eur Heart J 2009;30:2622–9.
ACCURACY (Assessment by Coronary Computed Tomographic
13. van Werkhoven JM, Schuijf JD, Gaemperli O, et al. Prognostic value
Angiography of Individuals Undergoing Invasive Coronary Angiogra-
of multislice computed tomography and gated single-photon emission
phy) trial. J Am Coll Cardiol 2008;52:1724 –32.
computed tomography in patients with suspected coronary artery
2. Miller JM, Rochitte CE, Dewey M, et al. Diagnostic performance of
disease. J Am Coll Cardiol 2009;53:623–32.
coronary angiography by 64-row CT. N Engl J Med 2008;359:2324–36.
14. Pundziute G, Schuijf JD, Jukema JW, et al. Prognostic value of multislice
3. Meijboom WB, Meijs MF, Schuijf JD, et al. Diagnostic accuracy of
computed tomography coronary angiography in patients with known or
64-slice computed tomography coronary angiography: a prospective,
suspected coronary artery disease. J Am Coll Cardiol 2007;49:62–70.
multicenter, multivendor study. J Am Coll Cardiol 2008;52:2135– 44.
15. Shaw LJ, Min JK, Narula J, et al. Sex differences in mortality
4. Min JK, Shaw LJ, Devereux RB, et al. Prognostic value of multide-
associated with computed tomographic angiographic measurements of
tector coronary computed tomographic angiography for prediction of
obstructive and nonobstructive coronary artery disease. Circ Cardio-
all-cause mortality. J Am Coll Cardiol 2007;50:1161–70.
vasc Imaging 2010;3:473– 81.
5. Min JK, Lin FY, Dunning AM, et al. Incremental prognostic
16. Abidov A, Rozanski A, Hachamovitch R, et al. Prognostic significance
significance of left ventricular dysfunction to coronary artery disease
of dyspnea in patients referred for cardiac stress testing. N Engl J Med
detection by 64-detector row coronary computed tomographic angiog-
raphy for the prediction of all-cause mortality: results from a two-
17. Diamond GA, Forrester JS. Analysis of probability as an aid in the clinical
centre study of 5330 patients. Eur Heart J 2010;31:1212–9.
diagnosis of coronary-artery disease. N Engl J Med 1979;300:1350–8.
6. Min JK, Feignoux J, Treutenaere J, Laperche T, Sablayrolles J. The
18. Diamond GA, Forrester JS, Hirsch M, et al. Application of condi-
prognostic value of multidetector coronary CT angiography for the
tional probability analysis to the clinical diagnosis of coronary artery
prediction of major adverse cardiovascular events: a multicenter obser-
disease. J Clin Invest 1980;65:1210 –21.
vational cohort study. Int J Cardiovasc Imaging 2010;26:721– 8.
19. Falk E. Morphologic features of unstable atherothrombotic plaques
7. Shaw LJ, Berman DS, Hendel RC, Borges NS, Min JK, Callister TQ.
underlying acute coronary syndromes. Am J Cardiol 1989;63:114E–20E.
Prognosis by coronary computed tomographic angiography: matched
20. Shaw LJ, Shaw RE, Merz CN, et al. Impact of ethnicity and gender
comparison with myocardial perfusion single-photon emission com-
differences on angiographic coronary artery disease prevalence and
puted tomography. J Cardiovasc Comput Tomogr 2008;2:93–101.
in-hospital mortality in the American College of Cardiology-
8. Hadamitzky M, Freissmuth B, Meyer T, et al. Prognostic value of
National Cardiovascular Data Registry. Circulation 2008;117:
coronary computed tomographic angiography for prediction of cardiac
1787– 801.
events in patients with suspected coronary artery disease. J Am Coll
21. Lloyd-Jones D, Adams R, Carnethon M, et al. Heart disease and
Cardiol Img 2009;2:404 –11.
stroke statistics—2009 update: a report from the American Heart
9. Hadamitzky M, Hein F, Meyer T, et al. Prognostic value of coronary
Association Statistics Committee and Stroke Statistics Subcommittee.
computed tomographic angiography in diabetic patients without
Circulation 2009;119:480 – 6.
known coronary artery disease. Diabetes Care 2010;33:1358 – 63.
22. Ostrom MP, Gopal A, Ahmadi N, et al. Mortality incidence and the
10. Hadamitzky M, Meyer T, Hein F, et al. Prognostic value of coronary
severity of coronary atherosclerosis assessed by computed tomography
computed tomographic angiography in asymptomatic patients. Am J
angiography. J Am Coll Cardiol 2008;52:1335– 43.
Cardiol 2010;105:1746 –51.
11. Chow BJ, Wells GA, Chen L, et al. Prognostic value of 64-slice
Key Words: atherosclerosis y computed tomography y coronary disease
cardiac computed tomography severity of coronary artery disease,
y nonobstructive y prognosis.
Source: http://www.debeerdejager.co.za/wp-content/uploads/2014/12/1-s2.0-S0735109711019541-main.pdf
Undergraduate Research Symposium The Auburn Montgomery School of Sciences Table of Contents Schedule of Events . 5 Poster Session I . 6 Oral Session I . 7 Poster Session II. 8 Abstracts . 9-28 Phagocytic Activity in Bufo marinus . 10 Antibiogram of Coliform Bacteria Isolated from River Water . 11 Anuran Immunology and the Effect of Corticosterone on Basophil Proliferation . 12
Ashok K A et al / Journal of Pharmacreations Vol-3(1) 2016 [40-63] Journal of Pharmacreations Pharmacreations Vol.3 Issue 1 Jan- Mar- 2016 Journal Home page: www.pharmacreations.com Research article Open Access New RP HPLC method for the simultaneous estimation of terbutaline