Ogp/ipieca 'guide to malaria management programmes' (2006)




A Guide to
Malaria
Management
Programmes
in the oil and gas industry


A Guide to
Malaria
Management
Programmes
in the oil and gas industry
IPIECA
International Petroleum Industry Environmental Conservation Association
5th Floor, 209–215 Blackfriars Road, London SE1 8NL, United Kingdom
Telephone: +44 (0)20 7633 2388 Facsimile: +44 (0)20 7633 2389
International Association of Oil & Gas Producers
London office
5th Floor, 209–215 Blackfriars Road, London SE1 8NL, United Kingdom
Telephone: +44 (0)20 7633 0272 Facsimile: +44 (0)20 7633 2350
Boulevard du Souverain 165, 4th Floor, B-1160 Brussels, Belgium
Telephone: +32 (0)2 566 9150 Facsimile: +32 (0)2 566 9159
This document was prepared by the Managing Malaria Issue Group on behalf of the OGP-IPIECA Health
committee. The Issue Group comprised: Alex Barbey (Schlumberger) (Chairman); Gary Krieger and Marci
Balge (Newfields); Alison Martin (BP); Gabriel Saada and Frano Mika (Eni Saipem); Jean-Pierre Gardair
(Total); Irene Alfaro (ARPEL); Laurent Arnulf (International SOS); David Johnson (Hess); Michele Alphonse
(ConocoPhillips); Philip Wiggs (IMCA); Brian Doll (ExxonMobil); Hans Berg and Geert de Jong (Shell).
IPIECA/OGP 2006. All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, ortransmitted in any form or by any means, electronic, mechanical, photocopying, recording or otherwise, without the priorconsent of IPIECA/OGP.
Disclaimer: Information provided herein is offered in good faith as accurate, but without guarantees or warranties of
completeness or accuracy. Readers are hereby put on notice that they must rely on their own diligence when determining how
or whether to respond to the information herein. Further, this guide is not intended to replace necessary and appropriate medical
or other professional advice or attention.
This publication is printed on paper manufactured from fibre obtained from sustainably grown softwood forests and bleached without any damageto the environment.
(The Appendices can be found on the CD-ROM which accompanies this document)
Purpose of this Guide
This Guide outlines and describes the scientific
issue that can transcend company medical
concepts, rationale and value of Malaria
support systems and significantly affect
Management Programmes (MMPs) for the oil
environment, safety and human resources
and gas industry. The Guide provides a broad
activities. The management of malaria is
overview of MMPs, and templates such as imple-
therefore a potential concern throughout the
mentation checklists and audit protocols that
supply chain of global exploration, production,
might typically form part of key activities when
refining, distribution and marketing.
implementing MMPs in the oil and gas industry.
This Guide attempts to build on successful
Experience within the oil and gas industry
industry practices. However, experience at
suggests that health is one of the key issues for
both the international health level, and from a
both the project workforce and the host
private sector perspective, indicates that
country. Health impacts can potentially occur
malaria management is both complex and
within defined project geographical bound-
difficult.There is no unique set of strategies or
aries and across surrounding communities.The
set of programmes that will work in all situa-
possibility of impacts is particularly true for an
tions or geographical locations. The only
issue like malaria that involves a complex
constant feature of both the biology and
interaction between biological and environ-
human medical science of malaria is change
mental variables and social and behavioural
and evolution. However, there are reasonably
practices. The oil and gas industry operates
well-understood principles that can be utilized
across a myriad of countries and cultures that
in virtually all situations that the oil and gas
form part of this interaction. Typically, the
industry is likely to encounter. This Guide
focus on malaria impacts is centred on Sub-
presents and analyses these principles and illus-
Saharan Africa (SSA), however, malaria
trates how they can be applied systematically
transmission occurs globally. Regardless of
within the context of worldwide oil and gas
geographical location, the industry operates in
operations. A series of linked technical appen-
an atmosphere of heightened expectations,
dices is provided on the attached CD-ROM so
particularly related to health, social and
that readers who want greater scientific expla-
environmental practices.When present, malaria
nation and technical back-up will have a
can be more than a health management
readily available source of information. For
problem; it is increasingly recognized as an
completeness, a glossary is provided.
The overall situation:global burden of malaria
Malaria is not a newly emerging disease.There
contrast, there were minimal effects in those
is an extremely long history of human and
geographical areas that are characterized by
malaria parasite interaction spanning over
high levels of malaria endemicity.These obser-
10,000 years. Malaria parasite populations
vations are consistent with the documented
experienced rapid growth in Africa and spread
evidence that controlling malaria across large
worldwide following human population
geographical areas becomes progressively more
growth, migration and agricultural devel-
difficult as a function of increasing intensity of
opment. Similarly, malaria morbidity, mortality
and disability have changed and evolved over
In many geographical areas, particularly in
time and geography.
sub-Saharan Africa, there is intense but stable
Human malaria risk has fallen from
year-round transmission. Therefore, MMP
53 per cent to 27 per cent of the Earth's land
strategies that are highly successful in a
surface. Sub-Saharan Africa (SSA) accounts for
geographical setting of low transmission may
59 per cent of the global clinical malaria cases,
fail in areas characterized by entrenched, high-
Southeast Asia accounts for 38 per cent and
level transmission. Further complicating the
Latin America accounts for 3 per cent. The
situation is a significant movement of popula-
Western Pacific region (which includes China)
tions from rural to urban settings. For example,
has less than a 1 per cent burden, despite a
in sub-Saharan Africa, urban cities are growing
large population, because of marked reduction
by approximately 10 per cent per year. Urban
in transmission across China since 1975. The
malaria has different transmission character-
World Health Organization (WHO) estimates
istics due to the unique ecosystem of the city
that on a worldwide basis, there are 300–500
million clinical episodes per year.
For many companies, operations exist
While there has been a contraction in the
simultaneously across virtually all geographical
geographical limits of all-cause malaria trans-
settings; therefore it should be anticipated that
mission, the gains have been in areas that had
a variety of malaria management strategies
relatively low underlying levels of malaria
would be required. for a
endemicity. Endemicity is defined as the
brief history of the evolution of malaria distri-
probable presence of malaria transmission. In
bution and impacts.
Figure 1: Global malaria risk, as classified by the World Health Organization (WHO) 1
Group 1 = low risk countries
(no chloroquine resistance)
Group 2 = high risk countries
(moderate chloroquine resistance)
Group 3 = high risk countries
(high chloroquine resistance)
1 WHO risk classification is basedon the parasite's resistance to themost common antimalarialpreventive medication,chloroquine. Countries areclassified as low risk (Group 1countries) and high risk (Group 2and 3 countries).
Key factors to promote success:role of senior management
For industry, one of the most important
Box 1: The role of senior management
insights in malaria management is simply
recognizing that malaria is a key business issue
Senior management is in a key position to:
that cuts across multiple staff and line
functions. Because malaria management
articulate corporate objectives;
potentially requires a large effort, a prominent
translate these objectives into performance
leadership role by senior management
becomes an essential initial activity (see
require development of a system for
Box 1). While the development of an effective
performance monitoring;
MMP is a highly technical undertaking, the
articulation of a ‘vision' involving the impor-
hold all levels of management accountable for
tance of malaria related issues becomes one of
the most important first steps.
provide the necessary resources, both financial
MMPs are multi-dimensional issues
and technical.
affecting numerous stakeholders both inside
and outside the company. Malaria impacts,
either positive or negative, are potentially
visible at the in-country staff level and even at
national and international levels. Corporate
company and the host country: an effective
Social Responsibility (CSR) efforts, along
programme can significantly enhance
with company reputation, can be impacted by
operating efficiency and safety while providing
malaria. MMPs offer a significant oppor-
a clear positive benefit for the host country at
tunity for a ‘win-win' scenario for both the
multiple levels.
What are Malaria Management Programmes (MMPs)?
Malaria is a disease that involves the interaction
manage malaria illustrates that this disease
of a parasite, a vector and a host. A vector is
demonstrates remarkable resilience in human
defined as an organism that carries and transfers a
populations despite enormous efforts to eradicate
microorganism from one host to another. For
it. In order to realistically develop and implement
malaria, the host includes both humans and other
MMPs, it is necessary to construct a basic scien-
MMPs are multi-disciplinary,
tific framework that captures the underlying
integrated efforts that combine expertise and
biology, pathophysiology (how humans respond
strategies in human and vector biology, environ-
to malaria infection) and epidemiology of
mental management, clinical medicine and
malaria infection.This fundamental framework is
community level interactions to protect people
generally built around the principles of primary,
from malaria. The long history of efforts to
secondary and tertiary prevention.
Malaria Management Programmes—levels of prevention
For MMPs, the levels of prevention can be
specifically defined (see Figure 2) so that an
in tropical and subtropical areas and is the
integrated programme can be developed
predominant species causing severe and
potentially fatal disease;
Primary prevention is considered to be
Plasmodium vivax—found in Asia, Latin
eradication and is focused on vector
America, and a few areas of Africa. Because
control strategies.
of Asian population densities, this is the
Secondary prevention is controlling and
most prevalent form of malaria worldwide;
reducing risks. Secondary prevention
Plasmodium ovale—found primarily in West
strategies cover the full range of personal
Africa and islands of the western Pacific.
protection (including chemoprophylaxis
This form of malaria is similar to vivax;
and repellants) and behaviour modification
and can produce a long-lasting and chronic
Tertiary prevention is treatment of
infection with an extremely long duration.
disease in order to prevent impairment
and subsequent disability or death.
Life cycle of malaria
The female Anopheles mosquito is the key
Primary prevention of transmissible
vector for transmitting malaria parasites to
vector-borne diseases
humans because they require blood meals as a
source of protein for the production of eggs.
Two critical factors are:
a source of blood meals; and
Malaria is a parasitic disease of microorganisms
the feeding and resting behaviour pattern
that belong to the genus Plasmodium. While
of the mosquito (dusk or dawn versus
there are more than 100 species of Plasmodium
nocturnal (night time), as well as the
that can infect many birds, reptiles and
primary location of feeding and post-
mammals, there are only four species of
feeding resting, i.e. indoors versus
Plasmodium that typically infect humans:
Figure 2 Defences against malaria
behaviour and attitude
personal protection:
DEET, treated clothing,
insecticide treated bed nets
Malaria management programmes—levels of prevention
Feeding and resting behaviours have a
significant impact on both the overall vector
efficiency and the analysis of potential control
measures, e.g. insecticide treated bednets
(nocturnal, inside biting), indoor residual
spraying (indoor resting), or source reduction
(outside biting and resting).
Pathophysiology
The period of time between the infective bite
and clinically experienced symptoms
(incubation period) typically ranges from
7–30 days depending on the infective species
y between infective
bite and symptoms can cause diagnostic
problems and place expatriate workers at
without continuous immune (infected bite)
significant risk since they or their physician
stimulation, e.g. when on long-term expatriate
might not recognize that a new fever could be
assignment to a non-malarial area.
malaria, particularly if they are no longer in a
malarial area.
After multiple malaria infections, an
For oil and gas operations, the shift from rural
individual develops partial protective
to urban setting is critical for MMPs. It is quite
immunity. This individual does not have full
likely that there will be operations in both
immunity but rather is described as ‘semi-
urban and rural settings with frequent inter-
immune.' Semi-immune individuals can still
action between the two. Major oil and gas
be infected by the malaria parasite but are less
including offshore platform
likely to develop severe disease and generally
settings, generally require some level of urban-
lack the usual malaria symptoms commonly
centred technical and staff support. Therefore,
associated with typical clinical disease.
the urban environment is important for the
Expatriates, regardless of home country
industry since it is probable that large numbers
location, are usually considered as ‘non-
of technical staff will transit through locations,
immune', since they lack sufficient protective
e.g. airports, that are located in areas impacted
by malaria.‘Airport malaria', defined as malaria
The development of acquired immunity
acquired through the bite of an infected
tends to be location specific and usually results
mosquito by an individual without exposure
from long-term childhood exposure. An adult
to the vector in its natural habitat, has been
individual from one malaria endemic region
frequently reported and is expected to
may not be protected in a country that has a
increase. A similar transmission problem could
different spectrum and intensity of malaria. In
even impact offshore platform crews since
order to maintain effective levels of acquired
ships and helicopters can readily transport the
immunity, an adult individual must be
mosquito vectors. In addition, continuous
constantly exposed to malaria. As an example,
work operations also increase the exposure of
an employee whose home country is in a
individuals to nocturnal vectors. Finally,
malarial area and who has been considered
human knowledge, attitudes, beliefs and
semi-immune will rapidly lose this immunity
practices regarding malaria are important.
Malaria management programmes—levels of prevention
Urban malaria epidemiology
It is not well known if all of the standard
malaria prevention, management and control
strategies can be effectively transferred to
urban settings. While there is some evidence
that anopheline species are adapting to urban
aquatic habitats (e.g. water-filled domestic
containers, back yard gardens), there is concern
that misdiagnosis and subsequent inappropriate
treatment of malaria is occurring.
All fevers cannot be presumptively assumed
to be malaria in an urban setting. The typical
clinical protocols that are employed in the
countryside may not be valid in the city.
Malaria ‘fogging' in Kuala Lumpur, Malaysia
Research has shown that 50–70 per cent of the
fevers in an urban setting are not laboratory
proven malaria despite an initial clinical (non-
laboratory) diagnosis to the contrary.Within an
urban context, the cost-effectiveness of standard
vector control strategies is also unknown.
Primary prevention: vector control
Figure 3: Using vector control to reduce malaria transmission
Box 2: Three strategies for vector control
Vector control in malaria
1. Reduction of human-vector contact by:
‘stopping Anopheles—a moving target'
the use of bednets;
improvements in housing (screening windows, eaves and doors);
• identification
repellants for skin and/or clothing;
• resistance to
insecticide dispensers (mosquito coils, plug-ins); and
room preparation (spraying curtains, under bed, etc.).
2. Vector density reduction (treatment of vector breeding places).
Most anophelines cannot fly more than 4 km from their breeding sites, and
• environmental
• personal protection:
generally remain within 2 km. Larval control is critical and directed
- clothing
- breeding sites
- repellents
• environmental
- resting areas
source reduction by environmental management, i.e. drainage, flushing,
• community protection
filling and altering river and lake margins so that they are unsuitable foranopheline breeding;
larviciding using both chemical insecticides and those of biological
origin, generally administered in cycles, which may vary between 2 and10 weeks;
The general goal of vector control is to reduce
biological control using predators such as larvivorous fish.;
malaria transmission by:
space spraying of insecticides for rapid reduction of vector density:
i) decreasing the contact between humans
there are significant limitations to this method including difficulty of
and the relevant vectors;
night time application and poor penetration of fogs into the daytimeresting places of the vectors.
ii) reducing the vector population density;
Any larvicidal strategy must also consider potential environmental impacts.
iii) changing vector longevity.
3. Decrease adult vector longevity by:
indoor residual spraying (IRS) for indoor resting mosquitoes; and
The three basic strategies that are directed
community-wide use of insecticide treated nets (ITNs), particularly for
towards different links in the overall trans-
mission chain are summarized in Box 2.
Indoor residual spraying (IRS)
sum of the individual protection. ITN
community outreach programmes sponsored
The main purpose of IRS is to reduce the
by a project, while complex, are still likely to
survival of malaria vectors entering houses. It is
be simpler to support and maintain than a
of little use for control of malaria vectors that
community-wide IRS effort.
rest outdoors, particularly if they also bite
outdoors and do not enter the sprayed
structure. Similarly, larval control depends
upon extremely high coverage since even a
Space spraying is the most rapid method in
few temporary breeding sites may be sufficient
areas of high population density, however it is
to maintain high transmission levels.
an emergency control method and unlikely to
be the main vector control strategy due to the
Insecticide treated nets (ITNs)
known limitations of this technique and the
rapid recovery of the vector population.
As ITN coverage increases, there is an overall
A night-time fogging campaign (e.g. between
reduction on the vector population; hence the
22:00 and 04:00) will have the greatest impact on
effect on the community is greater than the
nocturnal indoor feeding and resting mosquitoes.
Secondary and tertiary prevention oftransmissible vector-borne diseases
other primary prevention vector control
efforts. An example of a malaria programme
implementation checklist is included in
Secondary prevention involves controlling and
reducing individual risks by using the full range
‘A' for awareness and education
of personal protection and behaviour modifi-
As part of a secondary prevention programme,
cation measures. These measures are divided
companies often provide workers who are
into a four-level pyramid of prevention often
going to travel or reside in potentially malarious
known as the ‘A-B-C-D strategy' (Box 3):
areas with consistent, standardized educational
materials and instructions before travel to
malaria risk areas.To be effective, this instruction
Box 3: Secondary prevention—the A-B-C-D strategy
typically needs regular reinforcement while
working in the malaria risk area.
for awareness and education of the risk of malaria. It requires:
a relationship between patient and physician;
‘B' for bites—personal protection
understanding of prevention strategies; and
awareness pre-travel, during travel and post travel.
Bite prevention at the individual level is based
for bites—use of personal protection measures. It requires:
on creating a physical and/or chemical barrier
an understanding of Anopheles behaviour, i.e. feeding and resting;
between the person and the vector. The effec-
wearing of proper clothing, e.g. long-sleeved shirts, long pants,
tiveness of these measures is shown in Table 1.
use of appropriate repellents, especially at twilight and on neck,
use of permethrin on clothes and bed nets; and
Table 1 Effectiveness of barriers
preparation of the room for sleeping.
Effectiveness (at typical compliance levels)
for compliance with chemoprophylaxis.
Use of impregnated bed nets
Reduces transmission by 68–95%
for prompt diagnosis of malaria and securing early treatment.
Permethrin treated clothing
Reduces likelihood of infection by 24–97%
Permethrin impregnated
Reduces bites by up to 99%
clothes in combination with
In preparation for travel overseas some
use of N,N,-diethyl-3-
companies have established a ‘malaria visa'
methylbenzamide (DEET)
programme.The malaria visa approach requires
that an individual perform specific educa-
Long sleeve shirts and
Reduces likelihood of infection by up to 62%
tional, behavioural (for example, spraying
clothing with insecticide, obtaining repellents,
Reduces likelihood of infection by up to 93%
spraying bet nets with insecticide), and chemo-
Use of DEET on exposed skin
Reduces likelihood of infection by up to 45%
prophylaxis (use of a specific medication in
order to prevent development of malaria)
Vector control measures,
If 100% use was feasible, this package of
activities before permission is given to enter a
including all of the above,
measures would virtually eliminate malaria risk
plus residual insecticide
malarious area on company business. This
spraying, space spraying,
strategy is potentially quite effective for short-
elimination of breeding sites,
term assignments and for individuals who are
larviciding, biological controland the use of air-
transiting known malarious areas. The malaria
conditioning, where feasible.
visa strategy can be effectively combined with
Secondary and tertiary prevention of
transmissible vector-borne diseases
is compliance with both the medication AND
Table 2: Effectiveness of commercially available repellants
personal protection measures.
Duration of coverage
Drug-based prevention strategies are based
on two key concepts:
prevention of infection—also known as
Picaridin (KBR-3023) 9.3%
causal prophylaxis; and
Soybean-oil based
prevention of illness—known as
Citronella based products,
Less than 20 minutes
These strategies work by killing the
parasites as they differentiate and develop in
either the liver and/or the red blood cell.
discusses the malaria life cycle
The overwhelming medical consensus on
and presents the underlying theory for these
bite prevention is to strongly recommend:
drug-based strategies. As with all drug
(1) insecticide (permethrin or deltamethrin)
treatment regimes, malaria chemoprophylaxis
impregnated mosquito nets; (2) permethrin
is a balance between risk and benefit.
treatment of clothing; (3) wearing of long-
Medications all have potential adverse effects,
sleeved shirts and trousers; and (4) use of
individual tolerability issues and cost consider-
repellants for exposed skin (e.g. DEET or
ations. Many individuals purchase ‘black
market medications' that may be cheaper but
A variety of skin repellants are commercially
are often ‘fakes' containing no active ingredient
available. These products vary significantly in
or lacking appropriate pharmacological
their effectiveness (see Table 2). There are
potency. Even if using established brand name
marked differences in the duration of activity
drugs from reputable suppliers it is critical to
for each product. Every product requires
understand that no chemoprophylaxis regime
reapplication; however, some products are far
is 100 per cent efficacious because of:
more long-lasting than others. In general, the
unpredictable drug absorption;
various DEET products are the most effective.
variable therapeutic plasma levels being
reached due to individual genetic
‘C' for compliance with
differences in metabolism; and
the presence of drug resistant parasites.
Chemoprophylaxis involves taking a specific
medication in order to prevent development of
malaria. Each medication has its own spectrum
of side-effects, dosage schedule of adminis-
tration and indications and contra-indications.
Drug branding, marketing and advisory guide-
lines are typically produced on a target country
basis, since resistance profiles are constantly
changing for the medications.The most current
guidelines for the target country should always
be consulted. In addition, appropriate local
medical experts can also be consulted.
Regardless of the medication, the key concept
PhotoLink/Getty Images
Secondary and tertiary prevention of transmissible vector-borne diseases
noted above, in some cases this is due to a small
percentage of non-compliant individuals who
do not take, or do not consistently take, the
Compliance drug testing regimes, using
urine testing for medication metabolites, have
been implemented by some companies in the
oil and gas industry as part of an overall
Malaria Management Programme. These tests
form part of contractual arrangements
between employer and employee and where
required for non-immune expatriate staff will
likely also be required for contract staff;
individuals testing negative for metabolites
The full range of secondary prevention
are first counselled and transferred to a
strategies should be considered for all non-
‘frequent test pool'. Should the problem
immune individuals.
persist, the individual will be investigated
individuals, the situation is more complex.
further to determine the cause of the
Chemoprophylaxis is often considered for:
problem and if necessary may be transferred
infants under three years of age;
to a non-malarial area.
semi-immune pregnant women;
semi-immune people who have left their
‘D' for prompt diagnosis and early
endemic malaria area for more than 6–12
months, becoming non-immune, and
Malaria is a true medical emergency that
returning to an endemic malaria area; and
requires rapid diagnosis and treatment, as
other vulnerable groups (e.g. people with
infected individuals can rapidly deteriorate
over a 24-hour period. Ninety per cent of
cases of all malaria are associated with:
It cannot be assumed that someone from a
inappropriate chemoprophylaxis, e.g. the
malaria endemic country is semi-immune since
wrong drug and/or dosage; or
partial immunity can only be acquired by signif-
icant and continuous exposure to the same
malaria species from childhood onwards.
Therefore, individuals transferring between
different malarious areas may need additional
medical consideration. Chemoprophylaxis alone
does not provide absolute protection; therefore,
providing the full range of secondary prevention
strategies is an important consideration.
Finally, with regard to compliance, it is
important to note that the provision of
antimalarials to employees in the field does not
obviate the risk of contracting malaria. While
in some cases this is due to poor absorption
and/or variable therapeutic plasma levels, as
Secondary and tertiary prevention of
transmissible vector-borne diseases
do not indicate malaria, travellers are
encouraged to take Coartem® as a precaution.
Coartem® is now included in the World
Health Organization (WHO) Model List of
Essential Medicines, and is being distributed
through the WHO as part of the worldwide
Roll Back Malaria initiative.
Some oil and gas companies have developed
RDT and SBT kits as part of their MMP
efforts. These kits represent tertiary prevention
and are not a substitute for developing a
In two-thirds of tropical travellers who die
comprehensive MMP that includes appro-
of malaria, either treatment is delayed or the
priate primary and secondary prevention. The
diagnosis is simply missed. In most cases the
essential features of comprehensive MMPs
individuals concerned never took chemopro-
involve systematic evaluation and institution of
phylaxis in the first place, so a common
primary and secondary prevention strategies so
recommendation is to assume that every
that an adequate and defensible wall of
traveller with fever or unexplained flu-like
prevention is constructed and maintained.
illness has life threatening malaria. This
recommendation will obviously produce
‘false-positives' and subsequent over-diagnosis
of malaria; however, the medical rationale is
that ‘false-negatives'
are potentially at
substantial risk for a fatal outcome due to
missed diagnosis. This overriding concern
related to delay in diagnosis has led to the
rapid diagnostic tests (RDTs); and
stand-by emergency treatment (SBT) kits.
When the test kit is well maintained, some
RDT products can achieve a sensitivity (the
ability to detect a ‘positive') for P. falciparum
similar to that obtained by microscopy. RDTs
can be damaged by exposure to high temper-
ature extremes (heat or cold). If transport and
storage within conditions specified by the
manufacturer are not met, the sensitivity of the
RDTs may be impaired and shelf life reduced.
Coartem® (artemether/lumefantrine), is a
new, life-saving malaria treatment that is
included in most SBT kits. Even where RDTs
Benefits of an MMP
A well-executed MMP can prevent morbidity
workforce (including semi-immune nationals),
and mortality in the workforce. MMPs send an
surrounding communities and other national
important and positive message to the entire
and international stakeholders.
Box 4: Benefits of a Malaria Management Programme
Protecting the health of the workforce
Demonstrating commitment of senior management to a key health issue
Defining roles and responsibilities between companies, contractors and host governments
Establishing an accurate and appropriate baseline of a key disease for future comparison during the development,operation and eventual closure of a project
Demonstrating the potential improvement in the malaria burden in surrounding communities
Identifying and documenting key environmental features that relate to vector habitat and subsequent control
Documenting baseline environmental conditions relevant to vector control
Developing and enhancing local, provincial and national capacity for malaria control
Providing a positive framework/opportunity for stakeholder input, involvement and trust building
Enhancing the companies profile amongst NGOs, international institutions, including multi-lateral development andfinancial institutions
Potentially contributing to host community's health systems capacity, infrastructure, and development
When to develop and implement an MMP
If a company is considering business opportu-
secondary and tertiary prevention practices
nities in malarious settings then, it is critical to
and procedures for any work in malarious
consider development of an appropriate MMP
areas, e.g. malaria visa process. In addition to
for all phases of the business activity.
their own workforces, these standard practices
Programme development and complexity
and procedures may cover a variety of
should reflect an accurate understanding of
contractors and suppliers.
malaria risks for company personnel and even
integrated approach, using primary, secondary
surrounding communities. Many companies
and tertiary prevention, is likely to have the
may wish to develop a standardized set of
greatest chance of success.
Integrating an MMP with other impactassessment and outreach programmes
Malaria is a multi-dimensional disease;
vector-related diseases like malaria as part of
therefore, a complex skill set is essential for
the impact assessment process. Integration with
programme development and management.
company HSE management and health risk
Construction of each level of the wall of
assessment processes is also important. Malaria-
prevention requires a diverse team of
related issues could be a significant area of
specialized professionals. If a proposed business
activity for both social and environmental
activity is in a malarious area, then the accurate
assessments. Because of both the importance
and detailed assessment of malaria risk is
and complexity of MMP issues, many
indicated. Experience indicates that environ-
companies in the oil and gas industry have
mental scientists,
developed stand-alone multi-disciplinary
professionals, vector biologists, education
integrated teams of specialists for programme
trainers and community development
development and implementation. Often the
specialists may be necessary. Malaria risks and
‘lessons learned' from MMPs in large projects,
impacts should also be considered in carrying
e.g. oil field development and pipelines, are
out health, social and environmental impact
directly transferable to both other key business
assessments.The OGP/IPIECA Guide to Health
partners and internally to other locations of a
Impact Assessments in the oil and gas industry
companies' worldwide business activity.
specifically discusses the need to consider
National and international stakeholder consultation
Malaria-related issues have a large and well-
carefully consider the multi-level social and
organized set of international stakeholders.
community ramifications of any compre-
These stakeholders include, NGOs, academic
hensive malaria management programme.
institutions, multi-lateral development and
finding agencies and institutions purely created
for malaria prevention, management and
control. In addition, some level of local,
provincial and national malaria control efforts
will be encountered at the host country level.
In many situations, co-ordination and commu-
nication with all of these international and
national stakeholders is a daunting task.
Nevertheless, because of the potential for
significant benefit or inadvertent adverse
impacts, e.g. duplication of efforts, unmet and
unanticipated community level expectations
that could be produced, it is important to
National and international stakeholder consultation
It has become apparent that significant
is increasingly asked to address problems that
advances in the medical and environmental
traditionally are ‘outside the fence line' and
control areas have not necessarily translated
historically considered responsibilities of the
into success at the individual, community and
host government. In a given project setting,
health systems levels. There is a significant gap
comprehensive secondary and tertiary
between intervention efficacy and effectiveness
prevention strategies may be adequate for the
at the community level in a developing
project; however, it is quite likely that other
country setting. Increasingly, the oil and gas
international and national stakeholders will
industry faces the need to understand
request a more active outreach role in all levels
community level health, social and environ-
of prevention management and control, partic-
mental concerns in order to receive and
ularly in vector control efforts. In order to
maintain a ‘license to operate.' MMP is a
realistically understand these expectations,
particularly difficult set of issues because the
careful, close and early consultation during
biology of the disease is not easily confined
project formation and development stages
within the boundaries of a proposed project
with key national and international stake-
and invariably, in a large project, overlaps into
holders is advisable.
adjacent communities.The oil and gas industry
Putting it all together: the MMP process
There is no single MMP process that will neces-
process and is illustrated in Figure 4. The
sarily be appropriate in all the diverse situations
process is modelled after the general framework
confronting the oil and gas industry. However,
used in the suite of environmental, social and
there are a series of systematic steps that can be
health impact assessments (see Box 5).
used in order to determine what type of MMP
is appropriate in a particular situation. Many
companies in the oil and gas industry already
Box 5: Framework for social and health impact assessments
have a general approach for developing MMPs.
Similarly, many international agencies and
Screening—determine if a proposed business activity is going to take
place within a potentially malarious environment
national governments have published detailed
Scoping—outline the range and types of malaria problems that could be
guidelines covering malaria diagnosis and
treatment at both an individual and community
Planning including resourcing, cost and time management—consider
level. Because both diagnostic testing and
the types of resources, activities costs and level of effort that may be
available medications and treatment protocols
are constantly evolving, the most currently
Stakeholder consultation—co-ordinate, communicate and exchange
information at the local, provincial, national and international level
available guidelines should always be consulted.
Risk assessment—investigate, appraise and qualitatively or quantitatively
While the science of malaria is constantly
rank the impacts positive or negative that could be produced
changing, an overall management framework is
reasonably well established and can be used in
Mitigation strategy—develop a written mitigation action plan
almost all situations confronting the oil and gas
industry.This structure consists of a sequence of
Implementation and monitoring—define roles and responsibilities
common elements that frames the MMP
Figure 4: The MMP process
project conception
design and engineering
identification of
stakeholder communication and consultation
Putting it all together: the MMP process
nationals, and community residents. If
primary prevention vector control
The geographical settings where malaria trans-
strategies are deemed critical, then a
mission exists are reasonably well known.
general series of sequential questions
Therefore, if a business activity is likely to
should be considered.The overall process
either be centred in or transit through a
for this effort is shown in Figure 5.
malarious area then, malaria should be
considered as a potential health concern. A
The output of the scoping exercise can also
description of the proposed business activity
be used as a basis for formally developing a set
covering location, size, workforce, surrounding
of terms of reference (TOR). Either internal or
communities, and operations is essential. This
external consultants, or a combination of both,
initial review will help determine the need and
can use the TOR.
level of MMP that may be required. Not all
business activities require comprehensive
MMPs. In many situations, companies have
developed a ‘malaria visa' programme that is
based on secondary and tertiary prevention
Figure 5: Decision-making process (Najera, 2002)
strategies incorporated into the ‘A-B-C-D'
programme discussed in earlier sections of this
Stratify area according to the disease burden and
Guide. Based on the initial screening, implemen-
epidemiology of transmission
tation of a malaria visa programme may be
sufficient for the workforce. However, it is
important to understand that this programme is
internally workforce focused and not fully trans-
Determine whether there is a role for vector control
in each epidemiological stratum and in
ferable to the large number of semi-immune
current local circumstances
individuals who may be living in communities
adjacent to the proposed business activity.
If there is a role for vector control
determine vector(s) in each stratum
Scoping is generally a process for outlining the
range and types of hazards and potential
For each vector implicated determine:
beneficial impacts. The overall types and
• breeding sites
categories of questions that must be addressed
• adult resting sites• blood feeding behaviour
are defined at this stage. At the scoping stage
the overall types of questions include:
• history of insecticide resistance
defining the type and endemicity level of
malaria, e.g. dominant Plasmodium parasite,
and whether it is stable or unstable;
Determine which method(s) of
considering whether different strategies
vector control is (are) suitable
will be required depending upon the phase
of the project, i.e. construction, operation,
Where the use of insecticides is essential,
defining the at-risk population including
select the method and timing of application
construction workers, contractors,
Putting it all together: the MMP process
Planning including resourcing, cost and
time management
After the general scope has been determined,
the planning process can begin. It is critical to
identify at the outset the types of resources
that may be required. Resourcing issues
require careful consideration since multi-level,
integrated MMPs draw expertise across many
disciplines. While many oil and gas companies
have large and sophisticated medical, environ-
mental and safety departments, it is quite likely
ofsky/Getty Images
that some level of outside specialty expertise
will still need to be considered, particularly
related to the implementation of primary
vector control strategies. For large projects,
even secondary prevention strategies require
cally identified and defined since it is quite
significant levels of active on-site clinical
likely that there will be multiple levels of
medical support for accurate diagnosis and
groups and organizations that will be both
treatment. If the proposed business activity does
interested, active and operating within the
not require an on-site medical function, it may
overall sphere of the business activity. Malaria is
still be advisable to identify appropriate local
a disease that has attracted worldwide attention
resources, including medical practitioners and
in virtually all areas where transmission is
hospitals with appropriate malaria expertise and
found. Therefore, it is highly likely that any
proposed project in a known malarious area
Implementing an MMP is potentially an
will already be subject to some level of NGO,
expensive undertaking and may require a
national or international intervention control
significant level of staffing. The level of staffing
effort. Given this reality, the opportunity for
is a function of the goals that the programme
miscommunication and duplication of effort is
wishes to achieve and the underlying level of
significant. Therefore, a malaria stakeholder
malaria transmission. Many programmes have
communication programme is often considered
overall global objectives that include achieving
as early as possible in the overall business devel-
a zero fatality rate while minimizing the risk of
opment cycle. This effort should be carefully
contracting malaria to the lowest practicable
planned and coordinated in a fashion that is
level. Potentially, these goals can be achieved
consistent with and responsive to overall
but an intense, integrated and sustained effort
using a variety of primary, secondary and
tertiary strategies is likely to be needed.
Risk assessment is the process that investigates,
appraises and qualitatively or quantitatively
Stakeholder communication and consultation
ranks the impacts, positive or negative, that
is a process of mutual dialogue and information
could be produced by a given activity. Many oil
exchange between the project and the key
and gas companies have internal risk assessment
stakeholders. Stakeholders should be systemati-
procedures and protocols covering health,
Putting it all together: the MMP process
is indicated. As previously discussed, the profile
of malaria in urban and peri-urban settings is
quite different than the intensity usually seen in
a rural environment. If new data is deemed
necessary, then a series of carefully defined
study questions should be developed. These
study questions are likely to cover vector
species, habitat, and density in addition to
objective burden of disease.
The ranking of potential impacts can be
considered from an individual environmental,
medical and sociological perspective or as an
integrated exercise. Since malaria is a disease
that operates at many levels, it may be more
environmental, social and safety aspects of a
efficient and meaningful to develop an
proposed new business project.These processes
integrated impacts ranking that considers not
can be applied to MMP efforts. In a given
only health but also social and environmental
geographical location, it is important to under-
effects. The degree of detail and sophistication
stand the specific biology, pathophysiology, and
of the ranking exercise is project specific. The
epidemiology of malaria that may be encoun-
literature on community level impacts of
tered. The level of malaria risk will vary
malaria is vast and varies significantly across
substantially both by geographical location and
different global locations. Impacts and effects
complexity of proposed project. An oil field
observed in sub-Saharan Africa should not be
development and pipeline is likely to require
assumed to be fully relevant for Asia or South
substantially more investigation and
America. For a large project, that is expected to
programme development than opening a small
last for many years, risk assessments frequently
marketing office or retail store. The risk
consider both the workforce and the
assessment process can capture these differences
and provide an appropriate way to rank impacts
so that they can be address in a priority fashion.
Two important considerations in the risk
assessment process are the evaluation of existing
Decision making establishes priorities and
data and determination of the need for new
begins the process of developing and dedicating
baseline information. Existing sources of infor-
appropriate resources. For episodic or small-
mation must be carefully reviewed for accuracy,
scale business activities the implementation of
relevance and completeness. All fevers are
existing standard practices may be entirely
actually not malaria even though in rural
sufficient, e.g. a malaria visa programme. For
malarious areas fever is ‘presumptively assumed'
large, long-term projects, many companies have
to be malaria and treated accordingly. Many
established dedicated multi-disciplinary malaria
studies have documented that malaria is
management teams in order to simultaneously
frequently misdiagnosed. If there is a concern
manage both internal and external malaria
that the project will impact the existing trans-
issues. Senior management support, both at the
mission pattern and burden of malaria, then
project and corporate level, is essential since
careful consideration should be given to
sustainable MMP programmes are neither
determine whether a new data collection effort
simple nor inexpensive.
Putting it all together: the MMP process
management capacity is critical. Building the
environmental, medical and social capacity and
The written MMP is the mitigation plan. This
sustainability required for an integrated
plan specifies how high and how thick the ‘wall
approach to malaria are neither simple nor
of prevention' is constructed. The MMP is not
cheap. Many malaria programmes initially
a static exercise but a ‘living document' that will
succeed only to fail at a later date, as primary
evolve and change over time. The programme
prevention vector control strategies are not
is likely to be a combination of both internal
properly maintained. Long-term planning and
workforce and external community needs.
commitment is essential since sustainable
Many of the most important concerns and
capacity development is a long and slow
controversies surround the key vector control
process. The role of contractors becomes quite
strategies of insecticide application, IRS, space
important since much of the day–to-day
spraying, ITNs, and larviciding. Finally,
activity is performed by rotating contractors,
emergency response and planning should also
particularly during the construction phase of a
be performed since there is no 100 per cent
project. Contractor roles and responsibilities
effective MMP programme and, in some situa-
can be assigned and specified during the initial
tions, immediate treatment and or evacuation
scope of work contract process.
may be indicated.
Ongoing staffing levels will also require
attention and consideration since MMP is not a
Implementation and monitoring
static process. It should be reasonably antici-
pated that unexpected swings in weather and
For comprehensive MMPs, one of the most
human migration patterns and activities will
critical aspects of the implementation plan is
occur. Both of these events can have profound
the division of responsibilities and timescales
impacts on malaria transmission within the
between the project and the host government
workforce and external communities.
at local, regional and national levels. Roles and
Development of a monitoring system for
responsibilities should be defined and clearly
the overall MMP effort is a critical component.
understood, particularly if the MMP efforts are
A monitoring system is designed to document
going to extend outside the project bound-
how the programme is affecting malaria trans-
aries. Therefore, an analysis of local, regional
mission. A variety of indicators can be
and national malaria infrastructure and
developed for this purpose. Similarly, standard
medical outcome indicators can de developed
covering diagnosis and treatment,
suspected, probable, confirmed and fatal malaria
cases.These medical data are important because
it provides an early detection system for
changes, negative or positive, in malaria trans-
mission. A sample malaria case investigation
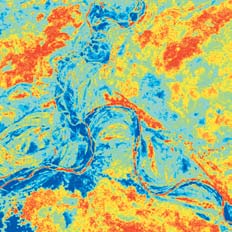
tesy of ExxonMobil
Left: satellite imagery can be used to predict the distribution
of the main vectors of malaria—landscape epidemiology is
a critical feature that can be used for the development of
Putting it all together: the MMP process
Finally, early detection is not the same thing
Audits should be considered at regular
as early warning. Malaria Early Warning
intervals because large projects are constantly
Systems (MEWS) require a different level of
changing, for example:
monitoring, planning and development and are
new company activities (e.g. work near
usually considered to be a national government
swamps, jungles, etc.);
project. However, because of the high levels of
new projects in potentially exposed
technological expertise, particularly regarding
geographic locations;
RS/GIS techniques, that are resident in many
modifications in work schedule (e.g.
oil and gas companies, collaboration or
technology transfer may be entirely appropriate
changing contractual requirements;
new scientific discoveries (e.g. medications,
international and government advisory
recommendations concerning malaria
Evaluation and verification of performance
resistance to medication.
and effectiveness is one of the most important
steps in an MMP programme. A system for
An example of an audit form is included in
determining that implementation has been
accomplished and is achieving the desired
results should be considered. Within the
implementation and monitoring plan a system
of outcome indicators is typically specified.
Auditing against these indicators can be
readily performed. Contractor performance
should also be verified and assessed for effec-
tiveness and compliance. If the MMP is
actively cooperating with host country
programmes, these efforts should also be
independently assessed against previously
established outcome indicators.
A variety of audit systems for health
programmes have been developed. General
audits often cover:
medical records and reports;
facility inspections for vector control
knowledge, attitude and practices (KAP)
training records—topics, attendances and
health care programme reviews and audits;
emergency drills; and
A simple way to remember the key steps
A mosquito bite that introduces malaria
needed to protect people from malaria:
parasites into the bitten host
Awareness - Bite prevention -
International Petroleum Industry
Chemoprophylaxis - Diagnosis
Environmental Conservation Association
Category (i.e. genus) of mosquito—some
Indoor Residual Spraying—treatment of
female species of Anopheles are capable
houses where people spend night-time
of transmitting malaria to humans and
hours, by spraying insecticides that have a
residual efficacy, i.e. they continue to
Size of a health problem in an area,
affect mosquitoes for several months
measured by cost, mortality, morbidity, orother indicators
Insecticide Treated bed Nets
A method of attempting to prevent
A parasitic disease that kills two million
malaria by taking various drugs prior to,
people per year around the world
during, and after exposure to malaria
Brand name of atavaquine-proguanil, a
A new, life-saving malaria treatment
drug used to prevent and treat malaria
A drug used to prevent malaria that goes
An insecticide (N,N,-diethyl-3-
under the brand name of Lariam
methylbenzamide) for use on exposed
Malaria Early Warning System—a system
skin to repel mosquitoes
for predicting malaria epidemics based on
A physical or mental impairment that
substantially limits one or more major life
Malaria Management Programme
Proportion of the population who have a
Exploration and Production
particular disease
Describes a disease that is localized to a
Proportion of a population who have
particular geographical region
died from a particular disease
The probable presence of malaria
An expert on insects, such as Anopheles
Term describing Anopheles mosquitoes
that are active at night
A sudden increase in the frequency of
A person with no immunity to malaria
malaria that significantly exceeds the
International Association of Oil and Gas
seasonal variation normally observed in a
A microorganism, such as Plasmodium,
The study of the incidence, distribution,
that lives, grows and feeds in a different
and control of disease in a population
organism while contributing nothing to
The human or animal in which the
the survival of its host
malaria parasite lives outside of the
Parasites (including those causing
malaria), bacteria, viruses or fungi that
Protection generated by the body's
can cause disease
immune system in response to previous
The functional changes in humans
malaria attacks resulting in ability to
resulting from infection by malaria
control or lessen a malaria attack
Incubation period
The interval of time between infection
Situation whereby malaria is spread
by a malaria parasite and the onset of the
throughout the year
first symptoms of the illness. Incubationperiods for malaria can range from 7 to
The area immediately surrounding an
40 days depending on the species
urban or city area
An insecticide effective in treating clothes
Stand-By emergency Treatment kits:
to repel and kill mosquitoes
these kits typically consist of two parts:(1) a Rapid Diagnosis Test; and
The category (i.e. genus) of the parasite
(2) malaria treatment medication such as
that causes malaria.The genus includes
Coartem; these kits enable personnel to
four species that infect humans:
self-test for malaria and take medication
Plasmodium falciparum, Plasmodium vivax,
to cure the disease.
Plasmodium ovale and Plasmodium malariae.
P. falciparum is the fatal form. P. vivax and
The widespread spraying of insecticide
P. falciparum are the species most
(often called fogging) from vehicles or
commonly encountered by the oil and
aircraft to kill mosquitoes
gas industry.
Sub-Saharan Africa
Prophylactic drugs
Medication taken to prevent malaria
Terms of Reference
Rapid Diagnostic Tests—these tests for
An organism (e.g. female Anopheles
malaria are often included in stand-by
mosquito) that transmits an infectious
emergency treatment kits to enable
agent (e.g. malaria parasites) from one
subjects to self-test for the presence of
host to another (e.g. humans)
malaria in their own blood.
Diseases (e.g. malaria) that are
The product of the chance that a specific
transmitted from one host to another
undesired event will occur and the
(e.g. humans) via an organism known as a
severity of the consequences of the event:
vector (e.g. female Anopheles mosquito)
Risk = (Probability) x (Consequence)
Process of eliminating mosquitoes thatcan transmit malaria
Remote Sensing/GeographicalInformation System
World Health Organization
List of Appendices
A ‘Guide to Malaria Management Programmes'on CD-ROM
This document is also included on the attached CD-ROM in PDF format†.The file includes links
to the associated Appendices which are also included on the CD-ROM. The links are represented
in this printed version by the blue underlined text.
† Requires Acrobat Reader™ — available from the Adobe w
* Web browser and Internet connection required
A Guide to
Al rights reserved. No unauthorized copies of this CD-ROM may be made without prior agreement with IPIECA/OGP
Malaria Management Programmes
in the oil and gas industry
This CD-ROM is designed to runautomatically. If it fails to start,browse to the file called ‘Malaria'and double-click to begin. (RequiresAdobe Acrobat Reader v.4 or later)
This CD-ROM contains the joint OGP/IPIECA publication
A Guide to Malaria Management Programmes in PDF format.
The PDF version includes links to related information
included on this CD-ROM.
The OGP/IPIECA Membership
Company members
ADNOC
AgipKCO
Hess
Anadarko Petroleum Corporation
BG Group
BHP Billiton
BP
Cairn Energy
Chevron
CNOOC
ConocoPhillips
Dolphin Energy
DONG
Denerco Oil
ENI
ExxonMobil
GNPOC
Hocol
Hunt Oil Company
Hydro
Japan Oil, Gas & Metals National
Corporation
Kuwait Oil Company
Kuwait Petroleum Corporation
International Association of Oil & Gas Producers (OGP)
Mærsk Olie og GasMarathon Oil
OGP represents the upstream oil and gas industry before international organizations
including the International Maritime Organization, the United Nations Environment
Programme (UNEP) Regional Seas Conventions and other groups under the UN
umbrella. At the regional level, OGP is the industry representative to the European
PetroCanada Petrobras
Commission and Parliament and the OSPAR Commission for the North East Atlantic.
Equally important is OGP's role in promulgating best practices, particularly in the areas
of health, safety, the environment and social responsibility.
PDOPetronasPetrotrin Premier Oil
International Petroleum Industry Environmental Conservation Association (IPIECA)
PTT EP Qatar Petroleum
The International Petroleum Industry Environmental Conservation Association (IPIECA)
is comprised of oil and gas companies and associations from around the world. Founded
Repsol YPFSaudi Aramco
in 1974 following the establishment of the United Nations Environment Programme
(UNEP), IPIECA provides one of the industry's principal channels of communication
with the United Nations. IPIECA is the single global association representing both the
upstream and downstream oil and gas industry on key global environmental and social
issues including: oil spill preparedness and response; global climate change; health; fuel
quality; biodiversity; social responsibility and sustainability reporting.
Association and Associate members
Australian Institute of Petroleum
American Petroleum Institute
ARPEL
ASSOMINERARIA
Baker Hughes
Canadian Association of Petroleum Producers
Canadian Petroleum Products Institute
CONCAWE
Energy Institute
European Petroleum Industry Association
Halliburton
Institut Français du Pétrole
IADC
IAGC
IOOA
M-I SWACO
NOGEPA
OLF
PAJ
Schlumberger
South African Petroleum Industry Association
UKOOA
WEG
Wintershall
World Petroleum Congress
Contents of this Guide:
The Appendices
Appendix A: Brief History of the Evolution of Malaria Distribution and Impacts
Appendix B: Primary Prevention of Transmissible Vector-borne Diseases
Appendix C: Secondary and Tertiary Prevention of Transmissible Vector-borne Diseases
Appendix D: Malaria Programme Implementation Checklist
Appendix E: Malaria Case Investigation Form
Appendix F: Audit Form
Pocket Guide to MMPs
Source: http://www.ipieca.org/?q=system/files/publications/malaria.pdf
This Provisional PDF corresponds to the article as it appeared upon acceptance. Fully formatted PDF and full text (HTML) versions will be made available soon. Proteomics reveals multiple routes to the osteogenic phenotype in mesenchymal stem cells BMC Genomics 2007, 8:380 Kristin P Bennett () Charles Bergeron Scott L Vandenberg ()
Track and Trace in the Pharmaceutical Supply Chain Edmund W. Schuster Visiting Operations Researcher Associate Director Massachusetts Institute of Technology husetts institute of technology, 400 technology sq, building ne46, 6th floor, cambridge, ma 02139-4307, usa Abstract The complexity of the United States health care system is increasing rapidly. Demographic changes, along with a host of new drugs, are causing greater volumes of raw materials and finished products to move through the pharmaceutical supply chain. Because drugs are expensive, there is always the possibility of counterfeit. Several recent cases of counterfeit medicines have raised American awareness of the problem. Information is an effective tool to combat counterfeit, however, new supply chain structures and relationships will need to emerge to organize and exchange information