Nzaht.org.nz
NZAHT FINGERPRINTS NEWSLETTER
Editor;
[email protected]
Position vacant: Editor of Fingerprints. Yes its official I am resigning after 9 fantastic years in the role. It is a role that keeps you in touch with the association and you get to read it all first hand! If you are interested in filling this role, come talk to me at the conference. This years conference; Hand TRAUMA 10-12 September, Langham Hotel. The guest speakers and timetable looks great and I‟m looking forward to it. Well done to the conference committee for a very professional job—glad to hear you are having a bit of fun along with the work. Fond farewell to our President Suzanne and thanks for being so great to work with. This newsletter is brought to you from the South.
Deadlines for next Edition
Cheers, Pam (Ed)
Northland and North shore
November—post conference
Many hands make light work
Executive Report…………………….2
ACC committee report……………….3
Education committee report…………….4
Christchurch Regional Rep….……….…5
Article review …………………………….6 article from our guest speaker at this years conference
Explain pain…………………………….11
Woundcare subjective assessment …….13
February/ March 2009 issue

NZAHT FINGERPRINTS NEWSLETTER
From the Executive
Exec Report August 2010.
The Exec are gearing up for the conference and look forward to seeing animated discussion on the website forum on the topics we have initiated and any others you wish to raise. This will allow us to plan ahead and move the NZAHT forwards as the world around us does so. We plan on making the website more user friendly and informative. We hope to see members participating in research. We wish to raise the profile of Hand Therapy. We want to provide scholarships for members to aid their personal growth and subsequently that of all our members. What would you like to see the NZAHT doing? How can you help to achieve this? The association is as strong as its members want to make it.
Suzanne, we wish you all the best. You are heading home to an exciting future. Thank you for all the time and effort you have put into the NZAHT. So much work done behind the scenes. You have lead and planned for a professional, dynamic and „learned‟ association. With a vision for the NZAHT that we will continue to drive. Doug, Eve and I have enjoyed your enthusiasm, friendship and leadership as we have come to terms with our roles in the NZAHT Exec. We look forward to hearing of your exploits in Europe and to seeing you back „down under‟ in the future.
With the conference looming, the ACC Contract submission in ACC‟s hands and many other issues being dealt with on a week by week basis it is a time to reflect on those whom put so many hours into our association. I am just coming to truly appreciate this and wish to thank everyone for all the work you do for us - the members.
See you in Auckland, in Spring! The daffodil shoots are searching for more sun so its not far off now. Craig Hawkyard President Elect Suzanne Koster President Evangeline Leys Secretary Doug Bryant Treasurer
February/ March 2009 issue
NZAHT FINGERPRINTS NEWSLETTER
ACC Committee Report
ACC Comittee update:
Firstly just to advise that we sent a comprehensive Submission to ACC as part of the review process for
the Hand Therapy Contract. Copies of full submission have been forwarded to Contarct Holders. Named
Therapists on contract wishing to read the full submission should apprach their Contract holder.
The Executive summary is included below for members.
Executive Summary (ACC Submission 2010)
The New Zealand Association of Hand Therapists (NZAHT) recognises the Accident Compensation
Corporation (ACC) Hand Therapy Services Contract is due for review in October 2010.
The NZAHT supports the continuation of the ACC Hand Therapy Services Contract, highlighting its
value over the past 10 years to ACC and its Hand injured clients. Under this contract ACC has the
benefit of contracting with named Registered Hand Therapists (RHT) guaranteeing post graduate
training, a specific level of experience and ongoing professional development ; which serve to
ensure a high quality, accountable service is delivered.
The NZAHT recommends variations to the current agreement to improve client access to services;
enhance the function of the contract and potentially save ACC time and money in duplication of
processes.
The proposed variations to the agreement include:-
a specific Prior Approval process be considered, for patients accessing post operative Hand
rehabilitation following ACC approved elective surgery. This would remove the need to
complete an ACC32 form for claimants with an already approved request for elective
surgery; thus eliminating the associated administrative delay between application and
approval of the rehabilitation. We believe this would be a cost saving measure for ACC,
given that 99% of these request are currently approved.
that any changes to the prior approval processes connected with this contract should be
Hand Therapy specific /sensitive see attached recommendations re the ACC32 process
( cf Appendix B)
An annual Consumer Price Index (CPI) linked, increase in Hand Therapy treatment fees paid
by ACC, to ensure sustainability of the service and thereby ensure timely client access to
treatment, thus optimising the return to work process and outcome.
An increase in the length of time allowed to complete the Hand Therapy Registration process
from two to three years to accommodate the recently increased time, workload and
financial demands on therapists working towards Registration.
The submission was fully supported by appropriate documents and it was particularly encouraging to recieve
many letters of support from surgeons and other referrers. Thankyou to al members who responded to our email
and forwarded our letter to their key referrers. It was well worth while.
Other apsects of the ACC review are underway, all contractors wil have recieved a questionaire form Simon Hoar
last month. We now await the outcome of the review and will keep you posted re developments.
We would encourage al practices to get prepared for completing outcome measures with ACC 32 from October
(we are recomending eithe QDash or PWRE), and to start thinking about computerised clinical notes as this is
likley to be a requiremnet in the future.
We are aware that ACC are definitely tightening up in the area of treatment numbers.
Our advice with the current ACC32 system is to be proactive; submit in good time and with as much supporting
evidence as possible ie OM, copy of treatmmnet plan or notes, op notes , surgeons letters etc. and to request
realistic treatment numbers .
NB .ACC have been doing some work with regard to Read Codes with respect to the Interim Physio Contact ie
with any code that does not have a TT profile defaulting to 6. Check with your PMS system as this should not yet
apply to Hand Contract and HT TT profiles should stil apply .
Final y just to advise that SIMON HOAR has moved to a different area in ACC and our Contact will now be
managed in the interimby Russell Elleswei . Russell usually looks after other Al ied Health providers including
Acupuncturists, Osteopaths, Chiropractors, Orthotics and Podiatry. We have a teleconference planned in next two
weeks when we hope to meet the new programe manager and get an update re the Contract.
Just a reminder that ACC will be sponsoring the AGM breakfast at Conference and will be presenting on the
(Continued on page 4)
February/ March 2009 issue
NZAHT FINGERPRINTS NEWSLETTER
Return to Work Programme (sorry exactname escapes me). Becausese of the tight time frames ,
we would ask that questions to the ACC presenter are limited to the topic presented.
Any questions related to the Contract should be emailed or adressed to the ACC
committee directly, and we wil collate and discuss any issues at the conference Emerging
Issues Forum (or a seperate Contract forum if required) and the take to ACC through our
teleconferneces . We feel this is important in light of the sensitivity of contracting
processes.
Julie Rouse pp. ACC Comittee.
Julie Rouse Sue Sewell Lisa Hansen Robyn Baldwin
Education Committee Report Education Committee
August Fingerprints 2010
Alice Cornforth and Donna Hickmott organized a highly successful Mulligan Workshop
which was held in Auckland August 7th. It was a 'hands-on' workshop with Brian
presenting some of his techniques for the upper limb joints and cervical spine. The course
was well attended and great to have a workshop that appealed to many of our more
experienced HT. We were honoured to have Brian Mulligan himself as the presenter and
the day was clinically useful, highly entertaining and with the scrumptious catering it did
not feel like a hardship to be at a course on a weekend! Many thanks to Alice and Donna.
The Education committee have all been continuing with their individual jobs and we have
kept in touch via email and one teleconference to date. The case studies and HAULT
continue to be under the excellent care of Rebecca and Edel respectively. Alice has
organized the workshop mentioned above. Our goal has been to have one workshop a
year, held at a different time to conference. If you have any ideas or requests for
workshops please let us know. Alison is involved with an OT working party focusing on
some continuing education and professional issues facing the OT HTs currently.
We are keen to have a new member join our committee so if you are interested in
continuing education - let one of us know. See you all in Auckland for conference.
Jackie Chiplin
Alice Cornforth
Alison Derbyshire
February/ March 2009 issue
NZAHT FINGERPRINTS NEWSLETTER
Canterbury Branch NZAHT
2010 has seen a change in tact from previous years with invited speakers appearing at each
in-service arranged throughout the year. To date we have had Dr Tony Goh, a Radiologist
from CRG talk to us on relevant hand radiology and Bridgett Rood from USL have a prod-
uct demonstration and splinting „knowledge sharing‟ evening. In late July Rebecca Kerner, a
Psychotherapist, will be discussing her role in the rehabilitation of appropriate clients that
we may see. This will be in conjunction with feedback from Lorimer Mosely‟s Explain Pain
seminar that Sara Lister and I attended. Later in the year Dr Sally Langley will be presenting
on Congenital Hand Conditions with Linda O‟Neill and Kerry Cragg feeding back on a
Paeds Conference they attended late last year.
A recent family trip to Rarotonga gave me an opportunity to help out a cousin who was there
for a year assisting the physiotherapy service. The locals were most appreciative and Pare,
the local physio absorbed all I could tell her on managing hand conditions….along with hav-
ing to study for her ultrasonography exam. She has had a crash three month course from a
visiting Radiologist, and will soon be responsible for the large variety of diagnostics under
ultrasound examination! If you happen to be travelling that way and want to help out let me
know.
See you in Auckland come September.
Craig
NZAHT (Website) Forum and Conference Emerging Issues Forum
The Exec have started several forum topics on the website and we encourage everyone to
view them and have input into how you see the NZAHT moving forwards in the years to
come. Topics include outcome measures and ACC, resources of the NZAHT, ongoing edu-
cation, promoting HT and participation in research and the NZAHT…….so please partici-
pate, help us to help you, after all it is your association! Feel free to start your own discus-
sion topic/s. The info will be collated and we aim to have further in depth discussion at the
Emerging Issues Forum, particularly on research and scholarships. Thanks.
February/ March 2009 issue
NZAHT FINGERPRINTS NEWSLETTER
Article Review by Jo Fisk
In the run up to the conference, I thought I would review an article by one of the speakers.
Chinchalker SJ, Gan BS, McFarlane RM, King GJ, Roth JH.
Extensor quadrigia: Pathomechanics and treatment
Can J Plast Surg vol 12 No 4 2004; 174-178
Verdan (1960) was first to describe the concept of quadrigia in relation to the FDP. If one of
the tendons is fixed, the reduced amplitude will affect the adjacent tendon.
The same can happen with the EDC where a single muscle motors four extensor tendons.
The article discusses the biomechanics of normal digital extension. From a fully flexed posi-
tion, the central slip initiates PIP extension. As the PIP gains extension, the lateral bands mi-
grate dorsally causing tension at the DIP joint resulting in DIP extension. The intrinsic mus-
cles thorough the central slip and lateral bands continue to extend the PIP and DIP, while the
EDC pulls the sagittal bands proximally, extending the MCP.
Extensor quadrigia can occur due to EDC adhesion following metacarpal fracture, and zone
V / VI tendon repair. The article explains that the tethering of the tendon creates a pseudo
insertion. This creates a lag at the MCP due to the lack of amplitude of EDC distal to the
tethering. Also, if it involves the fourth or fifth ray, changes may occur at the CMC joint
(hyperextension) further promoting the quadrigia effect.
Extensor quadrigia following sagittal band laceration and juncturae tendinum rupture / atten-
uation occur as a result of ulnar subluxation of extensor tendon. Extension is therefore not
full and subsequently results in decreased excursion of the adjacent digits through distal ten-
sion on the juncturae tendinae.
Extensor quadrigia caused by MCP flexion contracture occurs due to reduced gliding of the
extensor tendons proximally.
Quadrigia mainly results in a decrease in extension of the MCP joints. The intrinsics shorten
as they are held in a shortened position and to compensate for loss of extension at the MCP,
the intrinsics put excessive load on the PIP joint, leading to a swan neck deformity.
Treatment
Early diagnosis and recognition of the cause is important.
In a metacarpal fracture, a metacarpal fracture brace can be utilised to encourage tendon
gliding and also to prevent hyperextension at the CMC joint. Introduction of intrinsic stretch-
es when safe to do so.
Following extensor tendon repair in zone V and VI, reverse Kleinert technique is recom-
mended to promote tendon glide (which I guess is an extensor assist). The use of a figure of
8 splint for the PIP joint can be used until full excursion is regained (to decrease the load on
the PIP joint and help prevent swan neck).
Flexion contracture of the MCP joint (except Dupuytrens) should be treated with serial static
or static progressive splinting and intrinsic stretches.
For long standing extensor quadrigia, associated with swan neck deformities, surgery is
February/ March 2009 issue
NZAHT FINGERPRINTS NEWSLETTER
probably needed BUT therapy including intrinsic stretches, splinting to prevent swan neck tendency and maximise EDC excursion will reduce associated contributing factors and make surgery simpler. I‟ve never really thought about this as a quadrigia until I read this article. The biomechanics of the hand is so complicated and this article reaffirms the need for us to have a really good anatomical knowledge so that we can work out what is going on, what structures are involved and how best to tackle it. I‟ve never thought about blocking the PIP to work more on proxi-mal excursion of the EDC but I quite commonly block MCP extension to transmit the force more distally. It does seem quite logical. I look forward to the conference and I wonder whether S. Chinchalker may talk about this in more detail.
February/ March 2009 issue

NZAHT FINGERPRINTS NEWSLETTER
Please send requests for articles to:
Joanne Fisk
Physiotherapy Department
Christchurch Hospital
Private Bag 4710
Fax: 03 364 0442
Phone: 03 364 0694
Please include the title, journal and year, vol etc.Any posted articles will cost $1 to
cover photocopying and postage. (make cheques payable to physiotherapy
dept, Christchurch Hospital) If I can send it online then it's free. Please make sure you
include your address with your request so I know where to send it to.
Online access to the Journal of Hand Therapy continues to be available. It can be ac-
cessed through the NZAHT website. Click on the link.
Make sure you click on the institutional access of Elsevier first and then proceed to
put in the username (adminnzaht) and the password (admin_nzaht). If you click on
the article you want to view and then enter the username / password it won't work.
The Journal of Hand Surgery is subscribed to in paper form only. You can only view the
contents online.
February/ March 2009 issue
NZAHT FINGERPRINTS NEWSLETTER
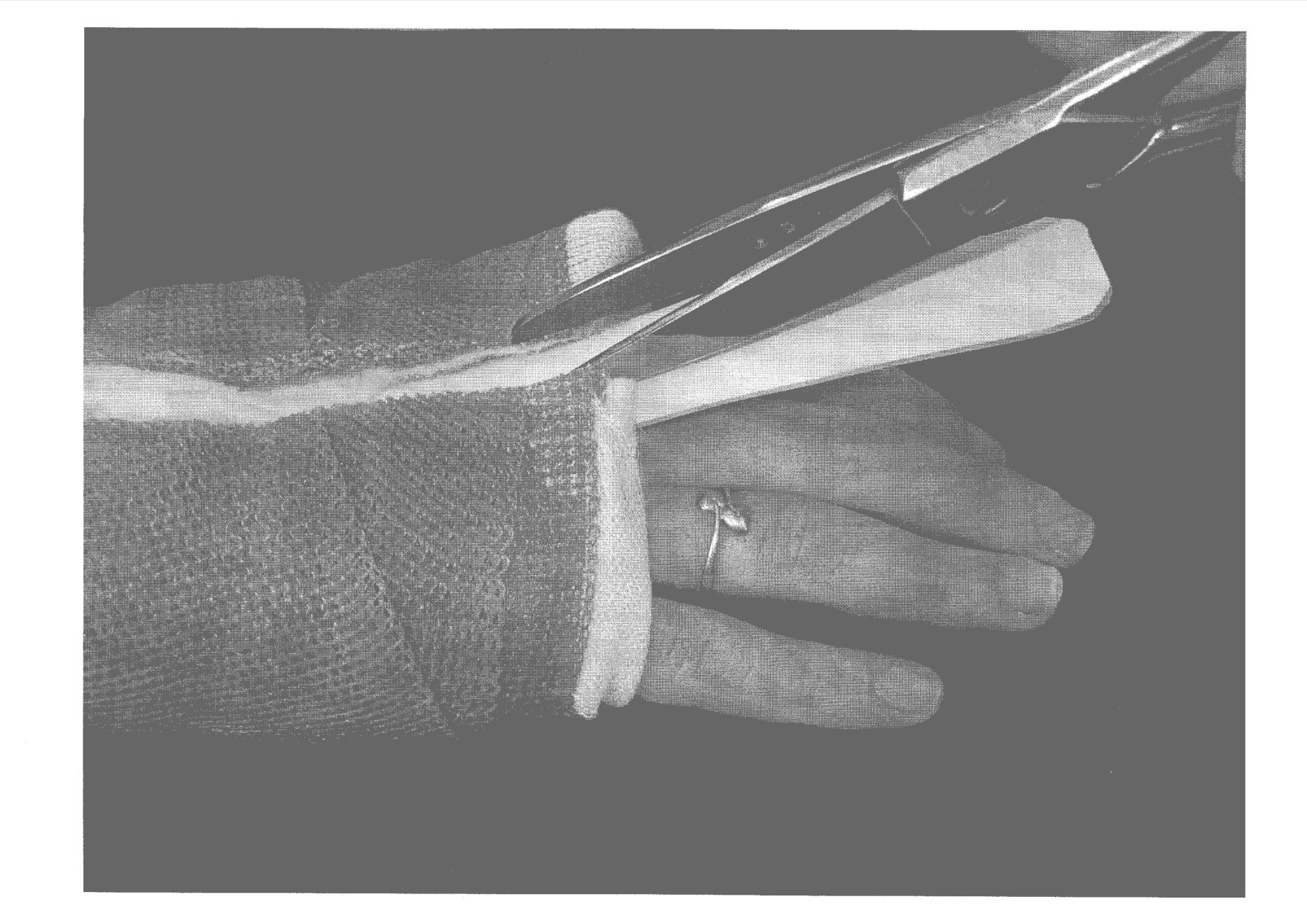
CLINICAL PEARL
When you are cutting off a soft cast splint, slide a thin "ruler" of thermoplastic
between the splint and the patient‟s skin first. Then you can safely cut away
knowing the patient‟s skin is protected from the scissors or plaster saw. The
patient can be asked to slide the "ruler" in to avoid catches on the skin.
Tjun Theng and Rebekah Kilgour
February/ March 2009 issue
NZAHT FINGERPRINTS NEWSLETTER
Explain Pain (and what its not)
Pain is a conscious correlate of the implicit perception of threat to body tissue. (Lorimer
Mosely)
Lorimer Moseley‟s recent presentation at the NZSP conference was a comical, up to date
and relevant session that would be of benefit to any Health Professional who deals with cli-
ents experiencing pain. I would highly recommend attending a course or at least reading the
publications that Lorimer and David Butler have researched, see noigroup.com or body-
inmind.com.au for further information.
Health professionals underestimate a lay person‟s ability to understand the complex neuro-
physiology of pain, yet the benefit of this information to a person suffering from chronic
pain has positive implications in their rehabilitation. Lorimer encourages clinicians to under-
stand currently accepted pain neurophysiology and to pass this on to their clients as part of
the rehabilitation process. Stories and anecdotes are liberally used in his presentation to help
get the message across. He encourages clinicians to develop their own, or better still have
the client relate their experiences to the underlying neurophysiology. i.e. „Biologising‟ the
physiology to reduce the personal stigma associated with pain.
Pain is an output of the brains evaluation and interpretation of a variety of factors, including
nociceptive input and other sensory cues, previous experience, context, beliefs and so on.
Our brain modulates nociceptive input from the periphery based on these factors, deciding
"how dangerous is this really?", to determine an appropriate output (of which pain may be
one of many). The pain makes us take action to promote our well being.
Nociception is neither sufficient nor necessary for pain.
Pain is not an accurate indication of tissue state.
Reflect back on some clients you have seen and I am sure you will see examples of this.
As pain persists the brain is likely to be contributing more to the pain state than nociceptive
input and the relationship between pain and tissue damage becomes more tenuous. Peripher-
al (detection system more sensitive, chemical soup) and central sensitisation (potentiation-
increased resting level of receptor excitation; intra-terminal genetic expression-gate facilita-
tion, a „doorstop‟ holds receptors open longer; soma genetic expression-gate production, and
they come unplugged for easier access) result in a system on red alert. That the brain modu-
lates nociception at the spinal cord is important because spinal cord adaptation (central sen-
sitisation) is important in the development of chronic pain. The brain becomes the orchestra
that plays the pain tune!
Lorimer aims to come in under this sensitised system, in the „its sore but its safe‟ zone.
Clearly defined flare up limits with an exposure baseline below this are set. Coping skills are
provided to help the client working in the „sore but safe‟ zone and he ensures they are clear
they are working well below tissue tolerance limits. Lorimer is also clear that this is part of a
larger management picture in which many other techniques may be useful.
A VERY brief overview of a fascinatingly complex subject matter, I hope it encourages you
to delve deeper as I think it is a very useful educational tool to have in your arsenal.
Craig
February/ March 2009 issue

NZAHT FINGERPRINTS NEWSLETTER
Wound Assessment: Subjective History
From 'Dunedin Hospital Hand Therapy Wound Care Guidelines, 2009'
Miranda Bühler BPhty NZRHT
History of presenting complaint includes mechanism of injury, treatment to date and pro-
gress made. A thorough history of the mechanism of injury is critical for complete appreciation of
severity of the wound. A small wound does not necessarily indicate a minor injury. For example
the high pressure puncture wound and the often tiny dorsal laceration resulting from contact with
a tooth. A crushing injury indicates a zone of tissue injury that may extend far beyond the obvious
skin defect. Such injuries may include compromise to the vascular system and thus impede wound
healing (Hunter et al., 2002).
Treatment to date should include the current wound care plan: who, when and how often wound
cares are being undertaken. Information on the progress to date may be gained from the patient
themselves or from clinical notes, with the aim of identifying whether wound healing is progress-
ing in a timely manner or has stagnated (Moffat & Vowden, 2008).
Date of injury and date of surgery(s) will anchor the time line from which phases of healing
can be predicted for both superficial and underlying tissues.
Age may impact on wound healing. Some significant changes have been shown to occur with in-
creasing age. The time taken for epidermal regeneration is increased from approximately 21 days
in young adults to 40 days for those in their mid-30s. The barrier function is reduced and the in-
flammatory response is weakened, increasing the likelihood of invasion by microorganisms and
subsequent infection. Vascularity of the skin is diminished, sensory perception is reduced, and
elasticity and tensile strength of the skin is reduced. Sensitivity of the skin can alter, increasing the
incidence of contact dermatitis (Flanagan, 1997).
Hand dominance will be of importance to the patient's functional capabilities during the period
of healing, and will be a factor in the degree of disability experienced from any long lasting prob-
lems.
Patients' current concerns may include wound odor and hygiene, and any barriers the wound
itself presents to participation in normal social and/or work activities (Moffat & Vowden, 2008).
Questions on social situation & lifestyle should give consideration to care environment e.g. in
hospital or the community; availability of support from professional or lay carers; availability of
wound care products and equipment; financial status (influences living conditions, balanced diet,
ability to afford care and specific treatments e.g. GP visits); substance abuse; major life stressors,
e.g. bereavement, separation, unemployment; and factitious injury (Moffat & Vowden, 2008).
Self care limitations may include issues such as sleep hygiene, adequate
self management of wound cares/hygiene, and cognition.
Work limitations/requirements may present a need for infrequent
dressing changes and therefore particular choices in wound care manage-
ment and products. A wound may be the limiting factor in RTW/function
and thus warrant more progressive choices in management including
dressings (Moffat & Vowden, 2008).
February/ March 2009 issue

NZAHT FINGERPRINTS NEWSLETTER
Leisure/sport may highlight that wound signs and symptoms limit so-
cialization. Sport and hobbies may make certain demands on types of
dressings (Moffat & Vowden, 2008).
Medical history should elicit any co morbidities that may prolong heal-
ing rates. Patients who are immunosuppressed are often unable to pro-
duce a normal inflammatory response and therefore may fail to activate
the normal process of healing. Medical conditions that may impair healing
include:
Circulatory disorder, e.g. anaemias, peripheral vascular disease, arteriosclerosis.
Respiratory disorders, e.g. chronic obstructive airway disease, bronchitis, pneumonia. Malabsorption disorders, e.g. Crohn's diseases, ulcerative colitis.
Metabolic disorders, e.g. diabetes, renal and hepatic failure.
Disorders of mobility and sensation, e.g. hemiplegia (CVA), paraplegia, neuropathy.
Immune deficiency disorders, e.g. rheumatoid arthritis, HIV/AIDS, cancer treatments (radiotherapy, chemotherapy).
Anxiety, depression
Smoker Allergy to dressing components e.g. adhesive
(Flanagan, 1997; Moffat & Vowden, 2008)
Medications: Anti-inflammatory and immuno-modulating drugs demonstrate impaired healing
at high doses in animal models however these findings are not consistently reproduced in clinical
trials in humans (Basti et al, 2005). It has been shown that these drugs affect inflammation and
local immune responses, which are necessary for proper wound healing and fighting off infection.
The continuation of these drugs during the early phases of wound healing is likely to be influenced
by individual factors. No consensus currently exists on their impact on the normal healing process
however they are listed here for consideration. There is agreement that steroids are more of a
concern particularly with regard to infection (Basti et al, 2005; Highton, 2009).
Corticosteroids, e.g. prednisone, methyl prednisolone
Non-steroidal anti-inflammatory drugs, e.g. aspirin, indomethacin, ibuprofen, diclofenac, naproxen Transplant suppressors, e.g. azathioprine
Disease modifying anti-rheumatic drugs (DMARDS), e.g. methotrexate, D-penicillamine, hu-
mera, leflunomide, gold sodium thiomalate, sulfasalazine, hydroxycholoroquine
Tumor necrosis factor-a receptor antagonists, e.g. etanercept, infliximab, adalimumab
Body chart includes symptom characteristics, behaviour and relationships. Pain in the region of
a wound or referred proximal or distal may be a sign of increased inflammation or infection. Pain
at dressing change is an indication for review of dressing choice (Flanagan, 1997; Moffat &
Vowden, 2008).
References
Basti, A. J., Hooper, J. S., Amaya, C. J., & Kazi, S. (2005) Effects of perioperative anti-inflammatory
and immunomodulating therapy on surgical wound healing. Pharmacotherapy – review of thera-
peutics.
Flanagan, M. (1997) Wound Management. Churchill Livingstone. London, UK.
Hunter JM, Callahan AD, Mackin EJ. Rehabilitation of the hand and upper extremity. 5th ed. St.
Louis: Mosby; 2002
February/ March 2009 issue
NZAHT FINGERPRINTS NEWSLETTER
Highton, Prof J. (2009) Personal communication 01.09.09, Dunedin, NZ. Moffat, C., & Vowden, P. (2008) EWMA position document: hard-to-heal wounds: a holistic ap-proach. London: MEP Ltd.
See you at the conference,
Signing off,
February/ March 2009 issue
Source: http://www.nzaht.org.nz/UserFiles/file/Fingerprints%20August%202010.pdf
& 2014 International Society of Nephrology A multicenter randomized trial indicates initialprednisolone treatment for childhood nephroticsyndrome for two months is not inferior tosix-month treatmentNorishige Yoshikawa1, Koichi Nakanishi1, Mayumi Sako2, Mari S. Oba3, Rintaro Mori4, Erika Ota4,Kenji Ishikura5, Hiroshi Hataya5, Masataka Honda5, Shuichi Ito6, Yuko Shima1, Hiroshi Kaito7,Kandai Nozu7, Hidefumi Nakamura2, Takashi Igarashi8, Yasuo Ohashi9 and Kazumoto Iijima7; for theJapanese Study Group of Kidney Disease in Children10
INESC MAT - Media Arts and Technology Description of the Research Project 1 Project Proposal 1.1 Summary of the Research Programme This research program aims at achieving innovation in various scientific and technological fields within the domain of Media Arts and Technology. Expected outcomes wil range from knowledge production (high-impact scientific publications and publications in the general media) to innovative prototypes and modular technologies of use to industry as wel as end-users. Media Arts and Technology (MAT) research fuses emergent media, computer science, engineering, and electronic music and digital art research, practice, production, and theory. This relatively new field of inquiry focuses on cultural content (music, video and film, TV, radio, performing arts, etc.) and its integration with the most recent Information and Communication Technologies, including the field of Human Computer Interaction. The research areas comprise a vast number of aspects ranging from multimedia processing and analysis, new media formats, content creation, searching, integration, adaptation, diffusion and presentation. The application domains of MAT range from improvements in conventional areas such as computer graphics, sound and music computing and artificial intel igence through enablers of new media industries up to new development of health therapies, education, fashion, and tourism, for example.