Astraco.co.th
Journal of Clinical Laser Medicine & Surgery
Volume 21, Number 3, 2003
Mary Ann Liebert, Inc.
Pp. 000–000
Two-Year Follow-Up Results of
Copper Bromide Laser Treatment of Striae
L. LONGO, M.D.,2 M.G. POSTIGLIONE, M.D.,1 O. MARANGONI, M.D.,2 and M. MELATO, M.D.3
Objective: The aim of our study was to follow-up 15 patients with stretch marks treated positively with the
CuBr laser (577–511 nm) in 1998–99 and followed-up for 2 years. Materials and Methods: The patients were
Italian women, young to middle age (average 30 years old), with skin coloration classified as Fitzpatrick II–III.
Biopsies were taken on some patients before the treatment and 1 month after the first treatment. Double-blind
histological, histochemical and photographic evaluation was performed. Results obtained as well as to the con-
tradictory effects reported elsewhere in the literature were compared. Results: On average, the results were
positive and there were some pathogenic considerations that justified the use of laser.
The effects of lasers on different phases of tissue repair have
been much investigated, including studies on the phases of re-
CUTANEOUS STRIAE, or stretch marks, are atrophic dermal epithelialization and collagen tissue formation. Some data is
scars with overlying epidermal atrophy. They are a cos-
now available.6–10 Given identical conditions and lasers,
metic defect but sometimes can be the sign of a true pathology.
dosage variations can cause opposite effects.11–13 Usually, a
Their etiology is often multi-factorial1,2 with constitutional
dosage of 2–4 Joules/per square centimeter on the tissue
in
causes: endocrine, metabolic, vascular, chronic inflammatory,
vivo and 4–20 Joules
in vitro stimulates fibroblast activity and
traumatic, iatrogenic and sometimes, neoplastic disorders.
the production of granulation tissues as well as active hyper-
There are multiple classifications of stretch marks following
emia and an increase in re-epitheliazation. These effects were
different criteria: color, morphology, etiology and age of striae.
revealed with 632–904-nm wavelength lasers and with
In accordance with these criteria, the striae are defined as white
380–1000-nm flash-lamps. By increasing the doses, the same
or red, superficial or deep, recent or old. No therapy has been
reparative procedures are inhibited, first reversibly and then ir-
codified until today and the results of all therapies are only par-
reversibly due to cellular and sub-cellular destruction caused
tially positive because only in exceptional cases do the striae
by the photo-thermal damage resulting in protein denaturation,
disappear totally. Different lasers have been proposed as a
micro-burns, macroscopic burns, carbonization and tissue ex-
treatment modality for this defect, but the results have always
plosion with vaporization.
been partial and/or lacking adequate follow-up.3,4 Furthermore,
Our earlier experiences in treating scar tissue led us to con-
the high cost of the instrumentation has prevented any system-
sider the use of lasers with wavelengths similar to pulsed
atic, wide-scale studies from being performed.
585 nm in the treatment of this cosmetic defect.
The flashlamp-pumped pulsed dye laser at 585-nm wave-
length has been used most frequently, using an energy densityof 3–8 Joules per square centimeter, and successfully tested in
MATERIALS AND METHODS
the treatment of scars.5 More recently, incoherent intense pulsedlight has been used for the same lesions, with filtered wave-
We selected, in 1998–99, 15 early middle-aged women of
lengths of 515–550–570–590 nm and fluences of 30–55 Joules
phototype II–III (Fitzpatrick Scale), with stretch marks on the
per square centimeter measured output. This modality is still
breasts, abdomen, dorso-lumbar region, and at the base of the
under clinical investigation.
lower limbs. The patients interrupted any other treatment
1General Surgery Institute and Phlebology Center, Siena University, Siena, Italy.
2Institute Laser Medicine, Florence, and Fondazione G. Bassi Trieste, Italy.
3Flow-Cytometry Centre, Trieste University, Trieste, Italy
Longo et al.
2 months before the laser procedure and they were in good
current manuscript deals with follow up assessment and treat-
health. They underwent treatment with a copper bromide laser
ment above and beyond the data detailed in the original study.
at 577 nm (ProYellow+, Asclepion-Meditec AG, Jena) at tissue
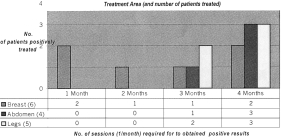
Three patients with breast strias and two patients with leg
doses of 4 Joules per square centimeter on the breasts, and
strias had the total disappearance of the strias (group of excel-
8 joules per square centimeter in the other regions. They were
lent results). The other patients had an improvement of the
treated with one to five sessions, 1 month apart, using a 1.5-nm
strias with reduction of dimensions and deep, more than 50%
spot diameter, with irradiation of the edges surrounding the le-
until 90% (group of good results).
sion. Overlapping of one-third between the spots was included.
Two patients had no positive results after the first four ses-
Off-time between the pulses was from 120 until 150 msec.
sions of treatment (group of less results). They decided to stop
The 577-nm laser was chosen because of its greater versatil-
the treatment. Two patients had results after two laser sessions,
ity as compared with the 585-nm pulsed dye laser. In fact, with
three patients after three sessions, and eight patients after four
the 577-nm laser it is possible to vary more parameters includ-
irradiations. Some photographic evidence is shown (Figs. 1
ing the duration of the pauses between laser pulses, and adapt
them to the individual case. In addition, 577 nm is the maxi-
The patients noticed a slight burning sensation during the
mum absorption peak of hemoglobin. The effects of the procedure that was immediately relieved with the desensitizing-577-nm laser have also been studied
in vitro.14
refreshing spray. After the procedure a slight sensation of heat
The dosage parameters applied in each irradiation15 are sum-
lasted for a few hours along with a little swelling of the treated
marized in Table 1. Before irradiation, the target zone was
area. There were also some transudation scabs that developed
cooled with a desensitizing cooling spray of Aloe Vera + Asia-
in the days following the procedure which lasted for about one
lene + Echinacea. A similar combination without Echinacea,
week. Some patients described mild, brief, but recurring pangs.
but with propylhydroxilic acid, in gel form, was applied for a
The stretch marks gradually changed in appearance over the
week after the session. No other substances were administered
course of one month. Then, if necessary, the patient underwent
before, during or after the treatment. Anti-inflammatory, and
further sessions spaced one month apart, for a maximum of
anti-erythema spray and cream were applied only for protec-
four sessions in eight patients.
tive purposes, during and immediately post-treatment.
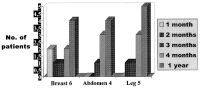
The follow-up after one year was positive (Fig. 2) because in
Histological and histochemical evaluation was performed on
13 patients out of 15 the results obtained were maintained and
3-mm-diameter punch-biopsies, including at the margin of the
it seemed that sun exposure had evened-out the skin appear-
striae and in tissue around the lesion.
ance. The follow-up after 2 years confirmed the stability of the
The results were evaluated on the basis of the planimetry
results obtained at 1 year. For maintenance therapy at home
of the lesions measured before and one month after each
after obtaining the reported results, we suggested the use of a
treatment and the morphological appearance of the lesions—
cream (Stretch-Peel*), once a day on the regions were the
using photographs, with specific reference to the depth,
striae might re-appear with most frequency.
width, and color of the striae. The patients were evaluated
Ultraviolet wavelengths have the greatest effect on scars. It
after 1, 2, 3, 4 months and at 1 and 2 years. Results were di-
seems that 380 nm is the most active, but it is only available
vided in three groups: excellent, with total disappearance of
from high-energy lamps and there are no such wavelength
the stretch marks; good, with reduction from 50% until 99%
lasers. Lamps, however, do not permit precise dosage of the ra-
of the strias area; less, with reduction less than 50%; and
diation as they emit incoherent light; nor do they permit the de-
poor, without changes.
termination of a single wavelength.
Therefore, in the treatment of striae, 577-nm copper bro-
mide lasers are well accepted by the patients, free of hazards
and non-invasive. We have not established the exact number ofapplications required for each type of striae even though it
The total results listed in Figure 1 were published in 2000.16
would seem that stretch marks on the breast require fewer ap-
The data from the previous study are used as a baseline and the
plications than the thighs, abdominal and dorso-lumbar re-
Pulsed dye
e confirm all
text cita-
Repeat-pulse frequency
tions are as
you meant.
Irradiated points
Lesion and adjacent tissue
Procedure of irradiation
No. and spacing of sessions
Copper Bromide Laser Treatment of Striae
Patients treated and results.
gions. The reason may be that in those regions, the skin is
genesis, confirmed this effect of yellow laser light. The photo-
thicker and the striae almost always deeper. A histological
graphic evidence from this study also confirms it.
evaluation of the results was not possible because the amount
One thing, however, is certain: the 577-nm copper-bromide
of the tissue biopsied was less, so the histological and histo-
laser can greatly improve scarring especially in the remodeling
chemical findings were not precisely measurable. On the other
and re-epithelization phases, and this is already an encourage-
hand, the patients accepted the use of punch biopsy specimens
ment for the pursuit of striae reduction in further trials.
taken before, during and after the treatment, but they would nothave accepted biopsies with a diameter of 1 cm, which wewould have needed to obtain exact histological and histochem-
ical data of statistical significance. The few biopsies obtainablefrom such patients could also explain the contradictory histo-
1. Zheng, P., Lavker, R.M., Kligman, A.M. (1989). Anatomy of
logical results reported in the literature regarding laser treat-
striae. Br. J. Dermatol. 112, 185–193.
ment of striae.3,4,14,15
2. A rem, A.J., and Kirschner, C.W. (1980). Analysis of striae. Plast.
Reconstr. Surg. 65, 22–29.
3. McDaniel, D.H., Ash, K., and Zukowski, M. (1996). Treatment of
stretch marks with the 585 nm flashlamp-pumped pulsed dye laser.
Dermatol. Surg. 22, 332–337.
4. Brandt, F. (1996). Pulsed dye vascular laser for the treatment of
Copper-bromide (577 nm) laser treatment of cutaneous
striae distensiae. Clin. Update 2, 1–3.
striae has proven effective in this trial. Too often in the past this
5. Alster, T.S. (1997). Laser treatment of hypertrophic scars, keloids
cosmetic defect seems to have been remedied with causal and
and striae. Dermatol. Clin. 15, 419–429.
non-causal treatments but the results were always disappoint-
6. Mester, A.F. (1988). A scientific background of laser biostimula-
ing in relation to the optimistic forecasts. For this reason, we
tion. Laser I, 23–26.
examined our patients again after one and 2 years prior to sub-
7. Longo, L. (1986). Terapia laser. Firenze: USES.
mitting these definitive results. Fortunately, the results ob-
8. Lievens, P. Influence of infrared laser on the proliferation of fi-
tained remained the same after 1 and 2 years. At the same time,
broblasts and collagen fibers. J. Clin. Laser Med. Surg. (in press).
we hope that our positive clinical impressions will be con-
9. Lubart, R., Friedmann, H., Sredni, B. et al. (1993). Light and bryo-
statin, a protein kinase C activator, promotes proliferation of
firmed by broader, multi-center studies.
human epidermal keratinocyte cultures, in: Laser/optoelectronics
The impossibility of obtaining histological and histo-
in medicine. W. Waidelich and R. Hofstetter (eds.). Heidelberg:
chemical confirmation data limits the value of our data. On the
Springer Verlag, pp. 448–454.
other hand, in vivo radioimmunoassays to measure PIIINP val-
10. McCaughan, J.S., Bethel, B.H., Johnston, T., et al. (1985). Effects
ues carried out by some authors in the study of collagen neo-
of low dose argon irradiation on rate of wound closure. LasersSurg. Med. 5, 607–615.
11. Longo, L., Evangelista, S., Tinacci, G., et al. (1987). Effects of
diode laser silver arsenide aluminium (GaAlAs) 904 nm on heal-ing of experimental wounds. Lasers Surg. Med. 5, 444–448.
12. Abergel, R.P., Meeker, C.A., Lam, T.S., et al. (1984). Control of
connective tissue metabolism by lasers: recent developments andfuture prospects. J. Am. Acad. Dermatol. 11, 1142–1150.
13. Longo, L., and Corcos, L. (1991). Defocused CO laser therapy in
pathologic wound healing, in: Laser/optoelectronics in medicine.
W. Waidelich and R. Hofstetter (eds.). Heidelberg: Springer Ver-lag, pp. 408–412.
14. Glassberg, E., Lask, G.P., Tan, M.L., et al. (1988). Cellular effect
One-year follow-up.
of the pulsed tuneable dye laser 577 nm on human endothelial
Longo et al.
cells, fibroblasts and erythrocytes: an in vitro study. Laser Surg.
Address reprint requests to:
Med. 8, 567–572.
Leonardo Longo, M.D.
15. Ash, K., and McDaniel, D. (1999). Current therapy of striae dis-
Institute for Laser Medicine
tensiae with 585 nm pulsed dye laser, in: Cosmetic laser surgery.
Borgo Pinti 57
T. Alster and D. Apfelberg (eds.). New York: Wiley, pp. 289–305.
50121 Firenze, Italy
16. Longo, L., Piccinetti, A.L., Dalle Monache, G., et al. (2000). Laser
treatment of stretch marks: preliminary results, in: Laser Florence99: a window on the laser medicine world. L. Longo, A. Hofstetter,M.L. Pascu (eds.). Bellingham: SPIE Publisher, pp. 164–168.
Source: http://www.astraco.co.th/pdf/pdf_17022009_8104214.pdf
Patient Fact Sheet Bisphosphonate Therapyand the Oral Cavity Bisphosphonates. What are they? Bisphosphonates are a class of drugs that are used to prevent bone loss demineralization (weakening or destruction). These have been used since the 1970s, but technological developments in recent years have continued to reduce the frequency of dosage and made other
Evolution, 56(7), 2002, pp. 1331–1339 WITHIN- AND BETWEEN-POPULATION VARIATION FOR WOLBACHIA-INDUCED REPRODUCTIVE INCOMPATIBILITY IN A HAPLODIPLOID MITE F. VALA,1,2 A. WEEKS,3 D. CLAESSEN,4 J. A. J. BREEUWER,5 AND M. W. SABELIS6 Institute for Biodiversity and Ecosystem Dynamics, University of Amsterdam, P.O. Box 94084, 1090 GB Amsterdam, The Netherlands