Slide
Breast Cancer, Cancer and Surgery
The Condition:
Tumors in the breasts are not uncommon, especially after age 30. Tumors
may be cancerous (malignant) or non-cancerous (benign). Approximately one
in nine women will develop breast cancer. Early detection can be made with
regular, manual self-examinations of the breasts, but not all tumors can be
detected in this manner. Mammography (X-ray of the breast) can detect
tumors that manual examination cannot.
Tumors are often removed surgically and treatment of malignant tumors may involve
surgery, radiotherapy, chemotherapy - or a combination of two or three of these
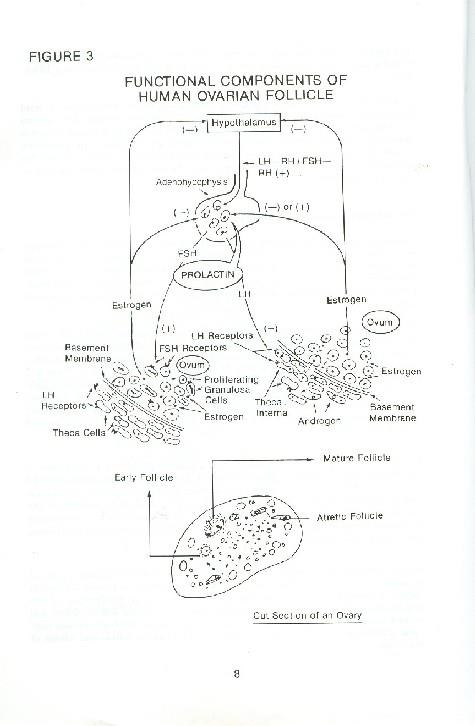
Ovarian Tumor
The Condition:
Ovarian tumors may be malignant (cancerous) or benign (non-
cancerous). Tumors may be solid or a hollow sac (cysts). Cysts are
sometimes filled with fluid and usually are the non-cancerous
form of an ovarian tumor. Ovarian tumors are not all that
uncommon and, if identified early, they can be removed surgically
or with radiation treatments.
Breast Cancer, Cancer and Surgery
Breast Cancer, Cancer and Surgery
Breast Cancer, Cancer and Surgery
Fitness and Diving Issues:
Cytotoxic drugs (chemotherapy) and radiation therapy can have unpleasant
side effects such as nausea and vomiting, and a prolonged course of therapy
can result in greatly decreased energy levels. This makes diving while
experiencing such side effects inadvisable. Radiation and some
chemotherapeutic drugs can cause pulmonary toxicity.
An evaluation to establish the safety of a return to diving should include an
assessment of the lung to ensure that damage likely to predispose the
diver to pulmonary barotrauma (arterial gas embolism, pneumothorax or
pneumomediastinum) is not present.
Finally, before diving, healing must have occurred, and the surgeon must be
satisfied that immersion in salt water will not contribute to wound
infection. Strength, general fitness and well-being should be back to
normal. The risk of infection, which may have increased temporarily during
chemotherapy or radiotherapy, should have returned to normal levels.
Pregnancy
Description of Condition:
Having a developing embryo or fetus in the body. Duration of pregnancy from
conception to delivery is approximately 266 days/9 months.
Fitness and Diving Issue:
There is little scientific data available regarding diving while
pregnant. Much of the available evidence is anecdotal. Laboratory
studies are confined to animal research and the results are
conflicting. Some retrospective survey type questionnaires have
been performed but are limited by data interpretation.
An issue to keep in mind is the risk of decompression illness to the mother due to the physiological changes which
occur while pregnant. During pregnancy, maternal body fluid distribution is altered, and this redistribution
decreases the exchange of dissolved gases in the central circulation. Theoretically, this fluid may be a site of
nitrogen retention. Fluid retention during pregnancy may also cause nasopharyngeal swelling, which can lead to
nose and ear stuffiness. In regards to diving, these may increase a pregnant woman's risk of ear or sinus
squeezes. Pregnant women experiencing morning sickness, which could then couple with motion sickness from a
rocking boat, may have to deal with nausea and vomiting during a dive. This is an unpleasant experience and could
lead to more serious problems if the diver panics.
Due to the limited data available and the uncertainty of the effects of diving on a fetus, diving
represents an increased exposure for the risk of injury during pregnancy. There's a baseline incidence
of injury including cases of decompression illness in diving. One must consider the effects on the fetus
if the mother must undergo recompression treatment.

Pregnancy
Diving and Pregnancy Outcome
Bangasser Survey 1978 - no increase defects
Bolton Survey 1980 - 109 women who dived prior to pregnancy,
69 stopped when pregnant higher rate of defects in groups who
continued including two major cardiac anomalies multiple
hemivertabrae, absent hand, VSD, coarctation, pyloric stenosis,
birthmark - no major defects in group that stopped (but no
higher than the general population and may be influenced by
Turner Case Report 1982
-twenty dives in 15 days, days post LMP 40-50
-most less than 60 ft., three dives 100 ft., one 110 - one rather rapid ascent from 60 ft., three dives
100 ft., one 110 - one rather rapid ascent from 60 ft.
-Sudafed also taken
-multiple anomalies
-head circumference normal, development normal, karyotype, EMG, muscle biopsy normal
-mechanism of DCS injury - fetal embolism or bubbling.
Please remember that one anecdotal report
does not create a syndrome or disease !
Animal studies of DCS during pregnancy also have noted increases in cardiac
malformations. If a woman dives inadvertently before pregnancy is diagnosed
during the first trimester of pregnancy, acknowledging that a very limited
amount of literature and experience exists, I suggest getting a second
trimester ultrasound (sonogram) with emphasis on limb and spinal development
and with good detailing of the cardiac structures and the configuration of the
great vessels around the heart -- aorta, pulmonary arteries, etc.
Return to Diving After Giving Birth
The Condition:
Diving, like any other sport, requires a certain degree of
conditioning and fitness. Divers who want to return to diving
postpartum (after having a child) should follow the guidelines
suggested for other sports and activities.
Fitness and Diving Issues:
After a vaginal delivery, women can usually resume light to moderate activity within one to three
weeks. This depends of several factors: prior level of conditioning; exercise and conditioning during
pregnancy; pregnancy-related complications; postpartum fatigue; and anemia, if any. Women who have
exercise regimens prior to pregnancy and birth generally resume exercise programs and sports
participation in earnest at three to four weeks after giving birth.
Obstetricians generally recommend avoiding sexual intercourse and immersion for 21 days
postpartum. This allows the cervix to close, decreasing the risk of introducing infection
into the genital tract. A good rule of thumb is to wait four weeks after delivery before
returning to diving.
Return to Diving After Giving Birth
Fitness and Diving Issues:
After a cesarean delivery (often called a C-section, made via a surgical incision
through the walls of the abdomen and uterus), wound-healing has to be included in
the equation. Most obstetricians advise waiting at least four to six weeks after this
kind of delivery before resuming full activity. Given the need to regain some
measure of lost conditioning, coupled with wound healing, and the significant weight-
bearing load of carrying dive gear, it's advisable to wait at least eight weeks after
a C-section before returning to diving.
Any moderate or severe medical complication of pregnancy - such as twins, pre-term
labor, hypertension or diabetes - may further delay return to diving. Prolonged bed
rest in these cases may have led to profound deconditioning and loss of aerobic
capacity and muscle mass. For women who have had deliveries with medical
complications, a medical screening and clearance are advisable before they return to
Additional Information:
Caring for a newborn may interfere with a woman's attempts to recover her strength and
stamina. Newborn care, characterized by poor sleep and fatigue, is a rigorous and demanding
Return to Diving After Giving Birth
The Condition:
A mother may choose to breast-feed her infant while maintaining an otherwise
active life. This may continue for weeks or months, depending on the mother's
Fitness and Diving Issues:
Is it safe to scuba dive while breast-feeding?
From the standpoint of the child, the mother's breast milk is not unduly affected. The
nitrogen absorbed into the body tissues is a component of breathing compressed air or
other gas mixes containing nitrogen. This form of nitrogen is an inert gas and plays no role in
body metabolism. Although nitrogen accumulates in all of the tissues and fluids of the body,
washout after a dive occurs quickly. Insignificant amounts of this nitrogen would be present
in the mother's breast milk; there is, however, no risk of the infant accumulating this
From the mother's standpoint, there is no reason for a woman who is breast-feeding
her child to avoid diving, provided there is no infection or inflammation of the breast.
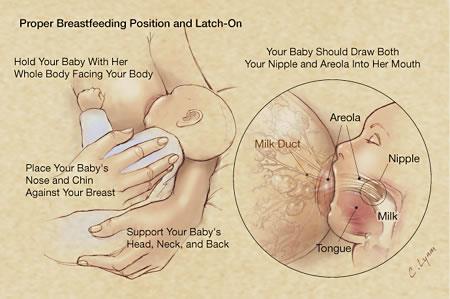
Beginning lactation
When the baby sucks, a hormone called oxytocin starts the milk flowing from the
alveoli, through the ducts (milk canals) into the sacs (milk pools) behind the areola
and finally into the baby's mouth
Return to Diving After Giving Birth
Breast Implants
The Condition:
Silicone and saline implants are used for cosmetic enhancement or
augmentation of the normal breast size and shape of reconstruction,
particularly after radical breast surgery for cancer or trauma.
In one study, by Dr. Richard Vann, Vice President of Research at DAN, mammary (breast)
implants were placed in the Duke University Medical Center hyperbaric chamber. The study did
not simulate the implant in human tissue. Three types were tested: silicone-, saline-, and silicone-
saline-filled. In this experiment, the researchers simulated various depth / time profiles of
recreational scuba diving. Here's what they found: There was an insignificant increase in bubble
size (1 to 4 percent) in both saline and silicone gel implants, depending on the depth and duration
of the dive. The least volume change occurred in the saline-filled implant, because nitrogen is less
soluble in saline than silicone.
The silicone-saline-filled type showed the greatest volume change. Bubble formation in implants
led to a small volume increase, which is not likely to damage the implants or surrounding tissue.
If gas bubbles do form in the implant, they resolve over time.

Breast Implants
Image displacement mammography
views (also called Eklund views) are
Standard mammography views are
performed with the implant pushed
taken first.
back against the chest wall. The
The breast and implant are
compression paddle is applied to the
compressed
breast tissue, which is pulled forward.
with moderate force
Silicone vs. Saline: Types of Breast Implants
There are two main types of breast implants, those that are saline-filled
and those that are silicone gel-filled. Each of these breast implants can
vary in shape, size, and shell texture. Some breast implants are pre-filled
for a set size, and others are filled through a valve during surgery. Some
types of breast implants even allow for filling adjustment after surgery for
size adjustment.
Breast Implants
Fitness and Diving Issues:
Once sufficient time has passed after surgery, when the diver has
resumed normal activities and there is no danger of infection, she may
begin scuba diving.
Breast implants do not pose a problem to diving from the standpoint of gas
absorption or changes in size and are not a contraindication for participation
in recreational scuba diving.
Avoid buoyancy compensators with constrictive chest straps, which can put
undue pressure on the seams and contribute to risk of rupture.
Additional Considerations: Breast implants filled with saline are neutrally
buoyant. Silicone implants are heavier than water, however, and they may
alter buoyancy and attitude (trim) in the water, particularly if the implants
are large. Appropriate training and appropriate adjustment of weights help
overcome these difficulties.
Menstruation During Diving Activities
The Condition:
Menstruation is the cyclic, physiologic discharge through the vagina of
blood and mucosal tissues from the non-pregnant uterus. The cycle is
controlled hormonally and usually occurs at approximately four-week
intervals. Symptoms may include pain, fluid retention, abdominal
cramping and backache.
Fitness and Diving Issues:
Are women at greater risk of experiencing decompression illness (DCI) while
menstruating? Theoretically, it is possible that, because of fluid retention and tissue
swelling, women are less able to get rid of dissolved nitrogen. This is, however, not
definitively proven.
One recent retrospective review of women divers (956 divers) with DCI found
38 percent were menstruating at the time of their injury. Additionally, 85
percent of those taking oral contraceptives were menstruating at the time of the
accident. This suggests, but does not prove, that women taking oral
contraceptives are at increased risk of decompression illness during
menstruation. Therefore, it may be advisable for menstruating women to dive
more conservatively, particularly if they are taking oral contraceptives. This
could involve making fewer dives, shorter and shallower dives and making longer
safety stops. Four other studies have provided evidence that women are at
higher risk of DCI, and in one study of altitude bends, menses also appeared to
be a risk factor for bends.
Menstruation During Diving Activities
Fitness and Diving Issues:
Are women at an increased risk of shark attacks during menstruation?
There are few reported shark attacks on women, and there are no data to
support the belief that menstruating females are at an increased risk for
shark attacks. The average blood lost during menstruation is small and
occurs over several days. Also, it is known that many shark species are not
attracted to the blood and other debris found in menstrual flow.
In general, diving while menstruating does not seem to be a problem as long as normal,
vigorous exercise does not increase the menstrual symptoms. As long as the menstrual
cycle poses no other symptoms or discomforts that affect her health, there is no
reason that a menstruating female should not dive. However, based upon available
data, it may be prudent for women taking oral contraceptives, particularly if they are
menstruating, to reduce their dive exposure (depth, bottom time or number of dives

Premenstrual Syndrome
The Condition:
Premenstrual Syndrome, or PMS, is a group of poorly understood and poorly
defined psychophysiological symptoms experienced by many women (25-50
percent of women) at the end of the menstrual cycle, just prior to the
PMS symptoms include mood swings, irritability, decreased mental alertness,
tension, fatigue, depression, headaches, bloating, swelling, breast tenderness, joint
pain and food cravings. Severe premenstrual syndrome has been found to
exacerbate underlying emotional disorders. Although progesterone is used in some
cases, no consistent, simple treatments are available.
Fitness and Diving Issues:
Research has shown that accidents in general are more common
among women during PMS. If women suffer from premenstrual
syndrome, it may be wise to dive conservatively during this time.
There is no scientific evidence, however, that they are more
susceptible to decompression illness or dive injuries / accidents.
Also, individuals with evidence of depression or antisocial tendencies should
be evaluated for their fitness to participate in diving: they may pose a risk
to themselves or a dive buddy.
Oral Birth Control
Description of Condition:
An effective and widely used method of preventing pregnancy.
There are several types of pills available and most contain a
combination of synthetic estrogen-like and progesterone-like
substances. These substances prevent the rise in luteinizing
hormone, which leads to ovulation. Also, oral contraceptives
thicken and chemically alter the cervical mucus, making the
uterine endometrium less receptive to sperm.
Possible side effects of oral contraceptives during the initial therapy include nausea,
vomiting, fluid retention, headaches and dizziness. Oral contraceptives may also be
associated with an increase in blood pressure and an increased risk of thromboembolic
disorders (development of clot-like vein occlusions, which can lead to an emboli).
Fitness and Diving Issue:
It has been suggested that oral contraceptives may increase a diver's susceptibly to DCS because of the
hormonal changes, which may reduce venous tone and increase water retention. This could affect circulation
and theoretically cause the blood to "sludge," which may interfere with the elimination of nitrogen from the
body. To date, no research has found evidence to support this belief.
In fact, unless oral contraceptives pose a clinical problem for women, there is no data to show that their
use during recreational scuba diving is a contraindication.
Oral Birth Control
Additional Considerations:
But what about contraception -- are there any specific hazards attached
to contraceptive methodologies which women and their consorts should
consider. Current thinking is that oral contraceptives do not impose any
increased risks on women divers. Most oral contraceptives used in the
USA carry a three- to four-fold increase risk of spontaneous non-fatal
thrombotic events, while pills containing desogestre (and gestodene, a
progestin commonly used in pills in the UK and other European countries
but not in the US) may carry a 6-8 fold increase in risk compared to no pill
use. When considering this increased risk of thrombosis, hyperbaric
researchers have been speculated that oral contraceptive use might
increase the likelihood of developing DCS or exacerbate the extent or
severity of tissue injury by promoting more rapid and profound activation
of the clotting cascade after a gas accident.
No animal studies have been done which support this hypothesis. On the contrary, one experiment of
DCS was done with pigs wherein half of the pigs were premedicated with oral contraceptives and then
subjected to chamber profiles inducing DCS injuries. The study found that extent of injuries was
identical in the treated and control pigs. No human epidemiologic surveys of sufficient sample size to
offer any information that is clinically useful have ever been done.
Recently the gynecologic literature has suggested that 50 percent of
thromboembolic on oral contaceptives may be due to interactions of the medication
with inherited clotting disorders, the most common abnormality being a protein
substitution in the chain of molecules forming clotting factor V. This substitution
renders factor V resistant to cleavage by activated protein C which would
inactivate its pro thrombotic action. The resultant disorder is called activated
protein C resistance.

Oral Birth Control
Additional Considerations:
Underlying coagulation defects have been implicated as increasing the
risk of DCS. As a matter of fact, heritable clotting disorders have been
implicated in idiopathic aseptic necrosis of the femoral head and a host of
other vascular complications. Those populations with a high incidence of
factor V Leiden mutation, the most common genotype responsible for this
coagulation defect, should be alert to and aware of clotting disorders.
Think of them when you encounter the unexpected, undeserved "hit" that
just seems too severe for the dive profiles when reviewing the diver's log
and history. And, of course, ask about oral contraceptive use.
Contraceptives Fact Sheet
Progesterone only pills, and long acting contraceptives (Norplant and Depo Provera)
The progestins, similar to those used in injectable contraceptives, all
progesterone mini pills, and implants, have effects on inflammatory cells. High
doses of progesterone have been found to help to stabilize cell membranes, and
thereby limit inflammatory response to injury. Women with sickle cell anemia on
high doses of progesterone have fewer and less severe sickle cell episodes. If
progestins act to limit inflammation, it might be postulated that they could help
limit the damage caused by the inflammatory processes that follow tissue
hypoxia in gas accidents. If true, we also might speculate that long acting or high
dose progestins might be the contraceptive of choice for women divers.
Barriers and Spermicides
Occasional questions arise about the possibility that the efficacy of barrier methods could be
reduced by immersion and dilution of the spermicidal agents if water washes in and out of the
vagina. The amount of flushing action in a wet suit is probably minimal; and obviously, is not a
consideration for dry suits.
Intrauterine contraceptive devices pose no hazard for the
female diver. Menstrual flow is increased in amount and
duration of flow. This can be a great inconvenience if a woman
is diving in a remote locale or on a boat with no sanitary
facilities or privacy.
Description of Condition:
To date, we have not had significant pool of women who:
- are post menopausal and at risk of osteoporosis
(menopause average at 50, osteopenia at 60-65, and
fractures starting at 70-75)
- have a significant diving experience including appropriate
number of dives at profound depth which put them at risk for
- therefore, we have no data on coincident osteoporosis and osteonecrosis in women at risk (or men for that matter).
Fitness and Diving Issue:
The pathophysiologic mechanisms leading to osteoporosis and osteonecrosis are
different. Osteoporosis results from decreases in osteoblast activity and
relative increase of osteoclast activity, resulting in bone resorption and
demineralization. The infarction of the microcirculation of bone is the
triggering mechanism for osteonecrosis.
Women are at increased risk for osteoporosis given that their overall lifetime
peak bone mass is lower than men and that the loss of estrogen during
menopause, greatly accelerates the rate of bone demineralization
All we can say at this point is that women should dive as conservatively as possible, thereby
trying to minimize their risks of osteonecrosis, so as not to impose this bone damaging
disease on top of their already increased risk of fracture due to Type I estrogen dependent
Source: http://www.nurkopedia.pl/images/e/ec/Women_and_diving.pdf
Prescribing Information RelaxaTM Polyethylene Glycol 3350 Powder for Oral Solution Red Leaf Medical Inc. Date of Preparation: 12 – 4055 Sladeview Crescent Date of Revision: <March 07, 2014> Submission Control No: 126786 RelaxaTM Package Insert Page 1 of 13 Table of Contents RelaxaTM Package Insert
For BROCK BIOLOGY OF MICROORGANISMS, THIRTEENTH EDITION Michael T. Madigan, John M. Martinko, David A. Stahl, David P. Clark Chapter 26 Microbial Growth Lectures by John ZamoraMiddle Tennessee State University © 2012 Pearson Education, Inc. Microbial Growth Control • Sterilization – The killing or removal of all viable organisms