Detailed report no action plan template

Primary Care Prescribing
Hywel Dda Health Board
Issued: August 2013
Document reference: 424A2013
Status of report
This document has been prepared for the internal use of Hywel Dda Health Board as part of
work performed in accordance with statutory functions, the Code of Audit Practice and the
Statement of Responsibilities issued by the Auditor General for Wales.
No responsibility is taken by the Wales Audit Office (the Auditor General and his staff) in
relation to any member, director, officer or other employee in their individual capacity, or to
any third party.
In the event of receiving a request for information to which this document may be relevant,
attention is drawn to the Code of Practice issued under section 45 of the Freedom of
Information Act 2000. The section 45 Code sets out the practice in the handling of requests
that is expected of public authorities, including consultation with relevant third parties. In
relation to this document, the Auditor General for Wales (and, where applicable, his
appointed auditor) is a relevant third party. Any enquiries regarding disclosure or re-use of
this document should be sent to the Wales Audit Office at
The team who delivered the work comprised Elaine Matthews, Sara Utley, Katrina Febry and
Page 2 of 70 - Primary Care Prescribing - Hywel Dda Health Board
Hywel Dda Health Board (Health Board) has made good progress setting the strategic direction for primary care medicines management, and could further progress the safety, quality and economy of local prescribing by making explicit links between strategy and action plans and strengthening organisational structures.
Our main findings
Strategic planning arrangements
The Health Board is to be commended on having a five year strategy for pharmacy and medicines management integrated across primary and secondary care with supporting actions and monitoring arrangements, although links between the annual prescribing plans and the strategy are not explicit
Structures, resources and managing the secondary interface
Insufficient staffing resources for primary care prescribing have been an issue but are now being addressed; the key medicines management groups need to further streamline their heavy workloads; and innovative initiatives are being piloted to improve interface working
Delivering safe, effective and economical prescribing
The Health Board has set realistic budgets and achieved financial savings from the primary care prescribing budget and can make further progress to support the safety, quality and economy of local prescribing
Appendix 1: Summary of potential savings
Appendix 2: Comparative analysis of BNF chapter prescribing by health board
Appendix 3: Analysis of prescribing indicators
Appendix 4: Reducing adverse drug reactions
Appendix 5: Managing drug wastage
Page 3 of 70 - Primary Care Prescribing - Hywel Dda Health Board
Appendix 6: Primary care prescribing diary exercise
Appendix 7: European Centre for Disease Prevention and Control (ECDC) key
messages for primary care prescribers
Page 4 of 70 - Primary Care Prescribing - Hywel Dda Health Board
Introduction
1.
The prescribing of drugs is the most common form of treatment in primary care and the NHS in Wales issues around 75 million primary care prescriptions each year amounting to around £600 million in medicine costs. The amount spent in primary care per head of population each year (£196) is higher than England (£169) and Scotland (£168). In addition the number of items prescribed in Wales for each person per year in 2012 is the highest in the UK at 24 items and this has increased from 15 in 2002.
This is set against a background of increasing demand and a high and increasing proportion of adults over 65 who generally receive more medicines. By 2020 the numbers are expected to increase by 24 per cent. In addition 82 per cent of this age group have a chronic condition which attracts higher prescribing rates.
The population covered by the Health Board is mostly rural although many people live in the small number of larger towns. A large proportion of the population has a life expectancy that is on average slightly higher than that of Wales and the mortality rate in people less than 75 years old is substantially lower than the rate for Wales as a whole. Population demographics do vary across the area and there are pockets of deprivation. The proportion of people with a long term limiting illness is just below average for Wales in Ceredigion and Pembrokeshire, but above average in Carmarthenshire.
The Health Board's Pharmacy and Medicine Management team is organised on a County basis, with each County team responsible for both secondary and primary prescribing. Each team is headed by a County Lead who is responsible for all activity relating to prescribing and other Health Board priorities. The Chief Pharmacist within the Health Board leads strategic developments for medicines management. Ultimately responsible is the Medical Director for the Health Board.
The last independent all-Wales audit of primary care prescribing was undertaken in 1998. The Auditor General has therefore included a review of primary care prescribing in his programme of local audit work at Health Boards in Wales. The Wales Audit Office carried out local reviews of primary care prescribing in Hywel Dda at each of the three Counties in 2009 and produced the report Prescribing at the interface between primary and secondary care in 2010. This audit has drawn on the findings from those earlier reports.
This audit examined the Health Board's approach to the management of primary care prescribing and sought to answer the question: ‘Is the approach being taken by the Health Board supporting safe, effective and economical prescribing within primary care?' by examining whether:
the primary care prescribing strategy and delivery plans support safe, effective and economical prescribing;
the structures, management arrangements and resources in place support secure safe, effective and economical prescribing; and
Page 5 of 70 - Primary Care Prescribing - Hywel Dda Health Board
prescribing data and financial outturns indicates that the Health Board's approach is resulting in the delivery of safe, effective and economical prescribing within primary care.
Our main findings
7.
Our overall conclusion is that the Health Board has made good progress setting the strategic direction for primary care medicines management, and could further progress the safety, quality and economy of local prescribing by making explicit links between strategy and action plans and strengthening organisational structures.
The tables below summarise the findings that have led us to this conclusion.
Strategic planning arrangements
The Health Board is to be commended on having a five year strategy for pharmacy and
medicines management integrated across primary and secondary care with supporting
actions and monitoring arrangements, although links between the annual prescribing
plans and the strategy are not explicit. We have come to this conclusion because:
Setting the strategic direction: the Health Board is to be commended on having a five
year strategy which supports the Health Board's overal shift of care from hospital setting to the community and its five core themes are robust. Detailed annual prescribing savings plans set a clear programme of work but the strategy's supporting actions are not SMART1, and have not been prioritised.
Use of evidence supporting strategy development: the strategy refers to global health
problems such as the increase in diabetes, and has identified appropriate actions to manage the entry of new drugs, although patient and stakeholder engagement was not used in its development.
Financial analysis used to support strategy development: the strategy refers to the
need for more controlled growth in the primary care drugs bill and detailed financial analysis supports the annual primary care savings plans.
Monitoring outcomes delivery and performance: the prescribing work stream monitors
delivery of the medicines management action plan and reports progress to the Medicines Management Group (MMG) and Integrated Governance Committee.
1 Specific, Measurable, Attainable, Relevant, Time-bound.
Page 6 of 70 - Primary Care Prescribing - Hywel Dda Health Board
Structures, resources and managing the interface with secondary care
Insufficient staffing resources for primary care prescribing have been an issue but are
now being addressed; the key MMGs need to further streamline their heavy workloads;
and innovative initiatives are being piloted to improve interface working. We have come
to this conclusion because:
Management arrangements: executive responsibility for medicines management is now
Prescribing support to primary care: pharmacist and technician roles in the County
prescribing teams are clearly defined and staff are working well with GPs, but there are significant capacity gaps which the Health Board is taking steps to address.
Health Board formulary: the Health Board has a complete formulary, which is available
across primary and secondary care and compliance with the formulary is monitored as part of the on-going support to GP practices by Health Board pharmacists.
Medicines Management Group (MMG): the MMG is well established as a subcommittee of
the Quality and Safety Committee and links to a number of important sub committees, although gaps in membership and attendance need to be addressed and the workload further streamlined.
Interface working between primary and secondary care: since our review of interface
prescribing in 2010, the Health Board has made improvements including to the quality of shared care protocols and innovative initiatives are being piloted to improve interface working.
Page 7 of 70 - Primary Care Prescribing - Hywel Dda Health Board
Delivering safe, effective and economical prescribing
The Health Board has set realistic budgets and achieved financial savings from the
primary care prescribing budget and can make further progress to support the safety,
quality and economy of local prescribing. We have come to this conclusion because:
Budget setting and financial performance: the Health Board sets its annual prescribing
budgets based on historic expenditure, growth and cost pressures. The target set for savings from primary care prescribing was £4.3 million in 2012-13 which was achieved at year end. Detailed information on meeting financial targets is prepared monthly and scrutinised by the MMG.
Overall expenditure on primary care prescribing: the Health Board currently spends
£65 million on primary care drugs and the spend is similar to the average for Wales when adjusted to take into consideration the numbers of older people in the population.
Indicators of effective prescribing: the Health Board has low levels of generic prescribing
and high levels of prescribing on preparations not recommended by NICE which indicates that, by targeting these and other areas highlighted in this report the Health Board could make additional annual savings of around £2.1 million without affecting patient care.
Prescribing on wound management, food supplements and incontinence products:
while the Health Board has been successfully targeting wound management and food supplements, there are still savings to be made by improving prescribing of these products.
National prescribing indicators (NPIs): the Health Board performs mid-range on most
NPIs and are better than average for prescribing morphine as a percentage of strong opioid items; but they are the worst for prescribing long acting insulin and below average on ACE inhibitor, proton pump inhibitor and hypnotic and anxiolytic prescribing highlighting the need to move the focus of prescribing support to these indicators.
Adverse drug reaction reporting (ADR): the Health Board has low compliance with the
Yellow Card reporting of ADRs and has recently appointed a Yellow Card champion to develop work in this area; but there are significant issues with the Datix adverse event reporting as GPs have disengaged from the process.
Drug wastage: medicine waste is highlighted on the risk register and the Health Board has
initiated a number of activities to reduce waste and make financial savings demonstrating its commitment to this area of work.
Page 8 of 70 - Primary Care Prescribing - Hywel Dda Health Board
Strategic planning arrangements
The Health Board needs to prioritise and revise the themes, aims and actions underpinning the Pharmacy and Medicines Management long term strategy to make them SMART so that they can be prioritised to the areas of highest impact and progress monitored effectively.
The Health Board needs to develop mechanisms to gather meaningful patient and stakeholder engagement to support the development of the primary care prescribing strategy and plans.
Structures, resources and managing the interface with secondary care
The Health Board needs to ensure that the arrangements for the MMG and its sub groups are appropriate, the representation by GPs is sufficient, and that the balance of work between the groups is optimised.
The Health Board needs to improve current discharge arrangements and develop standard discharge advice letters to ensure it has more effective care handover arrangements between consultants and GPs.
Delivering safe, effective and economical prescribing
The Health Board needs to develop a programme of work with GPs to deliver the potential savings identified in this report.
The Health Board should develop a medium to long term approach to delivering sustained improvements through education programmes and targeted prescribing advisor advice to GPs:
to improve ACE inhibitor prescribing;
to improve proton pump inhibitor prescribing;
to improve rational antibiotic prescribing; and
to reduce prescribing of dosulepin and hypnotics and anxiolytics.
Page 9 of 70 - Primary Care Prescribing - Hywel Dda Health Board
1. Strategic planning arrangements
9.
The Health Board is to be commended on having a five year strategy for pharmacy and medicines management integrated across primary and secondary care with supporting actions and monitoring arrangements, although links between the annual prescribing plans and the strategy are not explicit. We have come to this conclusion because:
Setting the strategic direction: the Health Board is to be commended on
having a five year strategy in place which supports the Health Board's overall
shift of care from hospital setting to the community and its five core themes are
robust. Detailed annual prescribing savings plans set a clear programme of work
but the strategy's supporting actions are not SMART and have not been
prioritised.
Use of evidence supporting strategy development: the strategy refers to
global health problems such as the increase in diabetes, and has identified
appropriate actions to manage the entry of new drugs although patient and
stakeholder engagement was not used in its development.
Financial analysis used to support strategy development: the strategy sets
out the aim for more controlled growth in the primary care drugs bill and detailed
financial analysis supports the annual primary care savings plans.
Monitoring outcomes delivery and performance: the prescribing work stream
monitors delivery of the medicines management action plan and reports progress
to the MMG and Integrated Governance Committee.
Page 10 of 70 - Primary Care Prescribing - Hywel Dda Health Board
10. The following tables summarise the findings supporting the conclusion.
Setting the strategic direction
Expected practice
In place?
Further information
The LHB has an up to date to
The Health Board has a medium term
prescribing strategy covering a
pharmacy and medicines management
defined period of time (for example,
strategy in place for 2011 to 2015. It aims to
three-five years), and associated
support the Health Board's overall shift of care
delivery plans to support
from hospital setting to the community. The
achievement of its strategic aims
strategy has five core themes:
with prioritised actions.
provision of patient centred care; reducing variation, harm and waste; delivery of value for money from investment
in medicines management;
communication and engagement; and development of a highly skilled, motivated
and flexible pharmacy and medicines management workforce.
Although the five core themes are robust the actions beneath are not SMART making it difficult to track when they have been completed. There are a significant number of identified actions, over 80, and there are overlaps within these. It is also unclear how some of the actions will address the core themes. While the strategy refers to a scoring system to prioritise actions, the current action plan has no evidence that the actions have been prioritised.
We understand that the detailed annual prescribing savings plans are targeted on actions that will make the greatest impact. While this means that the team has a clear work programme for the year ahead, its linkages with the strategy are not explicit.
The Health Board has in place a Prescribing Management Scheme. This was amended in 2012-13 to allow for part of any savings generated by GPs to be shared with other practices in each locality and provide new money to implement schemes of joint benefit. This approach is good practice although implementation has been slow.
Page 11 of 70 - Primary Care Prescribing - Hywel Dda Health Board
Setting the strategic direction
Expected practice
In place?
Further information
The Health Board's primary care
The Health Board's pharmacy and medicines
prescribing strategic approach
management strategy is integrated across
should be integrated with
primary and secondary care. The strategy
secondary care medicines
illustrates this integration by setting out the
management. In the absence of an
teams' responsibilities for all aspects of
integrated strategy the primary care
medicines management:
strategy should deliver a consistent
in-patient dispensing and patient
approach with its counterpart in
formulary development and providing
unbiased medicines advice to all prescribers;
undertaking medication reviews and clinics
in GP practices and care homes; and
close working with Community Pharmacy.
The strategic approach should link
The pharmacy and medicines management
to the Health Board's other
strategy reflects the strategic direction of the
strategic aims, for example its
Health Board's five year plan of providing care
Public Health Strategy.
closer to the community. Linkages are made to public health needs of the population, for example, the action plan proposes working with Public Health Wales and other organisations to support public health campaigns.
Planning arrangements address
Workforce is a theme of the pharmacy and
service redesign including
medicines management strategy and action
workforce developments and
plan, which sets out actions to develop the
pharmacy and medicines management structure and skills. A detailed assessment of Pharmacy and Medicines Management workforce needs was undertaken in January 2013. It sets out the requirements for additional capacity to meet the quality and savings agenda for the Health Board. The Corporate Decision Group made a request for additional funding for staff of £450,000 and amount approved was £355,000 PYE. Once recruited, the Health Board should have sufficient resources in place to make further improvements to the safety, quality and economy of local prescribing.
Workforce is discussed in detail in Section 2 of this report.
Page 12 of 70 - Primary Care Prescribing - Hywel Dda Health Board
Setting the strategic direction
Expected practice
In place?
Further information
Planning arrangements address
The pharmacy and medicines management
service redesign including effective
strategy is explicit that Community Pharmacies
use of community pharmacy
are a key partner in delivering effective
contract to deliver national and
medicines management and supporting the
local priorities for example local
health needs of the population in the
enhanced services.
community. Strategically the Health Board is using the community pharmacy contract to increase the amount of pharmacies offering an All Wales Enhanced Service, such as smoking cessation services.
The strategy addresses reducing
Through its action plan, the Health Board has
wastage for example through
identified the need to develop links with
promoting practice medicine
community pharmacy in respect of post
reviews, repeat prescription
discharge medicines reconciliation and
management and working with
encouraging uptake for repeat prescribing.
community pharmacists.
The Medicines Management and Prescribing
team support and encourage the uptake of DMRs and monitors uptake of DMRs by community pharmacies. Good progress is being made with 82 out of 99 pharmacies providing DMRs as at May 2013.
Use of evidence supporting strategy development
Expected practice
In place?
Further information
The strategy is informed by a clear
Although the core themes identified in the
analysis of factors influencing
pharmacy and medicines management
prescribing behaviour like
strategy are sound, and refer to global health
demographics, deprivation, needs
problems such as the increase in diabetes, the
assessment and public health
strategy does not demonstrate that it has been
informed by robust or comprehensive analysis of the Health Board's specific demographic and public health needs.
The strategy aligns with and
The pharmacy and medicines management
supports the delivery of national
strategy has an identified action which links to
policies regarding medicine
the development of established managed entry
including NICE guidance and
of new drugs in line with NICE and AWMSG
AWMSG guidance on the impact of
recommendations and supporting clinicians to
new drugs and changing use for
Page 13 of 70 - Primary Care Prescribing - Hywel Dda Health Board
Use of evidence supporting strategy development
Expected practice
In place?
Further information
The strategy aligns with 1,000 lives
The pharmacy and medicines management
and national service frameworks.
strategy refers to supporting clinicians to implement NSF and support and take forward the 1000 lives initiatives as part of the identified actions.
The strategy has been prepared
While the pharmacy and medicines
with input from key stakeholders
management strategy's first aim is ‘Being more
such as GPs, hospital consultants
responsive to the needs of patients and
and patient representatives.
service users through partnership and user involvement in service planning and delivery', none of the seven actions listed support this aim. The Health Board's MMG, where strategy, guidelines and savings plans are considered, has lay membership who have attended twice in the last year. The Health Board needs to develop mechanisms to engage with patients and stakeholders in the development of its long term strategy and plans.
Financial analysis used to support strategy development
Expected practice
In place?
Further information
The strategy includes a financial
The pharmacy and medicines management
analysis based on: historic growth
strategy contains no financial analysis
of the local drugs bill.
although it does refer to the need for more controlled growth in the primary care drugs bill. Detailed financial plans are developed on an annual basis based on historic growth and projected savings from the reduction in prescriptions for drugs targeted for reduction although longer term financial analysis is needed to support a five year strategy.
The strategy includes a financial
The pharmacy and medicines management
analysis based on: generic
strategy and action plan makes no reference to
prescribing and the use of branded
generic prescribing or use of branded drugs.
Even so, the Health Board is working with GPs to improve generic prescribing through, for example, switches to cheaper branded generics.
Page 14 of 70 - Primary Care Prescribing - Hywel Dda Health Board
Financial analysis used to support strategy development
Expected practice
In place?
Further information
The strategy includes a financial
The pharmacy and medicines management
analysis based on: the impact of
strategy refers to the development of a robust
new drugs and changing use for
mechanism for managing the introduction of
existing drugs including their impact
new medicines into clinical care which has
on existing care pathways.
been approved by the Quality and Safety Committee of the Health Board. Implementation plans are drawn up with Consultants and signed off by the MMG taking account of the financial analysis of the impact of new drugs and changing use of existing drugs on existing care pathways.
The strategy includes a financial
While the strategy refers to the significant
analysis based on: contingency
proportion of expenditure in secondary care on
arrangements for unplanned
high cost drugs, it does not set out any
developments for example using
contingency arrangements to address
high cost antibiotics if resistance
unplanned prescribing issues such as local
antibiotic resistance developing.
Monitoring outcomes delivery and performance
Expected practice
In place?
Further information
There are clear strategic aims,
The actions that underpin the pharmacy and
outcomes and SMART objectives.
medicines management strategy are not SMART and have not been prioritised. There is also overlap between some of the actions and they do not always address the core theme. The Health Board does have clear annual prescribing plans which set the work programme for the team but linkages with the longer term strategy and its actions are not explicit.
The framework for monitoring
The Health Board's prescribing work stream
delivery includes reporting to the
monitors delivery of the medicines
Board and appropriate Committees.
management action plan and reports progress to the MMG.
Page 15 of 70 - Primary Care Prescribing - Hywel Dda Health Board
2. Structures, resources and managing the interface with
secondary care
11. Insufficient staffing resources for primary care prescribing have been an issue but are
now being addressed; the key MMGs need to further streamline their heavy workloads; and innovative initiatives are being piloted to improve interface working. We have come to this conclusion because:
Management arrangements: executive responsibility for medicines
management is now clear.
Prescribing support to primary care: pharmacist and technician roles in the
County prescribing teams are clearly defined and staff are working well with
GPs, but there are significant capacity gaps which the Health Board is taking
steps to address.
Health Board formulary: the Health Board has a complete formulary, which is
available across primary and secondary care and compliance with the formulary
is monitored as part of the on-going support to GP practices by Health Board
pharmacists.
Medicines Management Group (MMG): the MMG is well established as a
subcommittee of the Quality and Safety Committee and links to a number of
important sub committees, although gaps in membership and attendance need
to be addressed and the workload further streamlined.
Interface working between primary and secondary care: since our review of
interface prescribing in 2010, the Health Board has made improvements to the
quality of shared care protocols and innovative initiatives are being piloted to
improve interface working.
Page 16 of 70 - Primary Care Prescribing - Hywel Dda Health Board
12. The following tables summarise the findings supporting the conclusion.
Management arrangements
Expected practice
In place?
Further information
There is clear professional and
Executive responsibility for medicines
managerial accountability for all
management is now clear following the
medicines management and GP
appointment of a full time Medical Director who
prescribing. This should include
has board level responsibility for medicines
executive lead at Board level.
management. The Health Board's Pharmacy and Medicine Management staff are based in three County teams each with a County Lead although not all posts have been filled. The teams are integrated across primary and secondary care.
Prescribing support to primary care
Expected practice
In place?
Further information
Primary care prescribing support
and advice roles are clearly
/ Pharmacist and technicians roles in the County
prescribing teams are clearly defined. When our
diary exercise data is analysed by County team (see Appendix 6), the time spent on the different activities varied. The amount of time spent working directly with GP practices was different across the three County teams with the Carmarthenshire team spending half their time with practices while Ceredigion and Pembrokeshire spent most of their time on Health Board activities. All teams predominantly work to support improvements to GP prescribing with a relatively small amount of time spent in the community and with secondary care.
Our audit found that the Health Board has fewer primary care prescribing staff than the average for Wales based on the adjusted population. This makes the delivery of the strategy and annual plans challenging. The Head of Medicines Management has filled this role on an interim basis for more than two years with no back filling of the vacated senior pharmacist post in the County. This is a risk on the medicines management risk register which shows that the Health Board recognises its importance. The Head of Medicines Management produced a report in December 2012 detailing the reasons for staffing issues in Pharmacy and Medicines Management and
Page 17 of 70 - Primary Care Prescribing - Hywel Dda Health Board
Prescribing support to primary care
Expected practice
In place?
Further information
making the case for additional resources. The Health Board has subsequently taken a paper to the Corporate Decision Group for additional funding to support the work of the team. If recruitment is successful this will increase the teams' capacity significantly and support the delivery of savings and the quality agenda.
Performance and compliance is
The Pharmacy and Medicines Management
monitored and prescribing team
team set targets for GP practices using a
resources are directed towards
formula based on patient need and deprivation,
priority and high impact areas.
which are achievable and should result in more support from GPs.
Targeting of support is undertaken based on those GP practices that have been identified where the greatest impact can be achieved. This is positive. However staff expressed concern that there was not enough staff to enable them to carry out all the work needed to realise the savings. Ongoing work to recruit additional resources should help to achieve further savings and improvements to quality of prescribing.
There are easy accessible data
Appropriate use is made of supporting
analysis and management
information systems to inform decision making
information systems and processes
and performance monitoring such as information
in place to support prescribing
from CASPA2 and the NPI. The team produces
this data showing comparative practice performance, which is shared at County meetings and with individual practices. CASPA currently is two months behind in real terms and the team would like more real time data.
The Health Board supports ScriptSwitch3 which is encouraging GPs to alter their prescribing practices, to comply with formulary and support generic prescribing. GPs interviewed were content to use ScriptSwitch.
2 Comparative Analysis System for Prescribing. Audit is an application for analysis of prescribing trends in primary care provided by NHS Wales Shared Services Partnership
3 ScriptSwtich is a UK wide tool supporting prescribing decisions, cost savings and patient safety
Page 18 of 70 - Primary Care Prescribing - Hywel Dda Health Board
Prescribing support to primary care
Expected practice
In place?
Further information
Primary care rational prescribing
education programme in place.
/ An education programme is in place through
continuing professional development (CPD)
events for GPs as part of the prescribing management scheme. There are also ad hoc training sessions run by the pharmacists. GPs would like more training and structured support which needs to be addressed by the Health Board although capacity to implement this remains an issue.
Health Board formulary
Expected practice
In place?
Further information
The establishment of a local
The Health Board has a complete electronic
formulary is an important tool to help
formulary, which is available across primary
provide information in support of safe
and secondary care and links directly to the
and economic drug choices within a
GPs' prescribing systems. A RAG status for
health board. In order to be effective,
drugs is in place, and identified clearly with
the formulary needs to be developed
drugs that are not suitable for management in
with the engagement of relevant
clinicians. It also needs to be
The formulary is not yet available for the public
promoted as widely as possible
to access via the internet although a freedom
across primary and secondary care,
of information request did result in the pdf
and should be made readily
version being placed on the internet in
available, including electronically.
The Health Board has established a
local formulary which identifies through a RAG (red, amber, green) system or similar process: Medicines suitable for primary
care prescribing.
Medicines initiated within a
hospital/specialist setting but suitable for shared care with primary care under a health board shared care agreement.
Prescribing responsibility lies with
a hospital consultant or a specialist.
Page 19 of 70 - Primary Care Prescribing - Hywel Dda Health Board
Health Board formulary
Expected practice
In place?
Further information
The Medicines and Therapeutic Committee does not recommend a
medicines use except in exceptional circumstances. In these instances prescribing adviser advice is needed and the reasons for prescribing recorded.
Formulary compliance is monitored
Compliance with the formulary is monitored as
and action taken when breaches are
part of the on-going support to GP practices by
Health Board pharmacists. GPs did not express any issues with compliance.
Medicines Management Group (MMG)
Expected practice
In place?
Further information
The work of local drugs and
therapeutics groups is a key
/ The MMG was established as a Sub
Committee of the Health Board's Quality and
component in ensuring safe, effective
Safety Committee in October 2010. The terms
and economical use of new drugs
of reference for the MMG list the membership
and types of treatment. The MMG
including a CHC representative to represent
membership effectively represents all
the stakeholders including lay
Our review of working papers found agendas
for the MMG are long. The Health Board has recently increased the number of meetings to cover the items although further work could be done to make the meetings more manageable.
The Health Board already has a number of workgroups which support the delivery of the MMG's workload: Antimicrobial Management Committee; Clinical Formulary group; Multidisciplinary Medication Event Review
NICE group; Non-Medical Prescribing Forum; Patient Group Directives Group; and Thrombosis committee. The lack of attendance of clinicians at the Medicines Event Review Group has prompted the Health Board to review its current arrangements.
Page 20 of 70 - Primary Care Prescribing - Hywel Dda Health Board
Medicines Management Group (MMG)
Expected practice
In place?
Further information
The pre-NICE group is a relatively new addition, created in response to an identified need for better scenario and impact assessment of new NICE drugs upon the Health Board. All medicines management activity (for example decisions from the MMG) is reported in detail to the Quality and Safety Committee where decisions are ratified.
The membership covers a wide
range of specialities in terms of
/ The MMG's membership does not fully reflect
the breadth of Health Board activities and has
medical expertise. This is necessary
insufficient clinical representation: Medical
to ensure that proper consideration is
Director, Associate Medical Director with
given to complex information in order
Responsibility for Medicines plus one Primary
that robust decision making can take
Care Medical Representative.
There is a GP representative on the Clinical
Formulary Group (where additions are made to the formulary) who actively participates in meetings.
Membership of the full MMG and sub groups needs to be reviewed and any gaps in membership addressed.
The forward plan sets out a work
The MMG Terms of Reference and Work Plan
programme for the year.
2012/13 from August 2012 clearly set out the group's standing items and work schedule for the year.
The MMG utilises the full range of
The MMG take into account comprehensive
information sources available to
information to support decision making and
inform decision-making.
monitoring of performance. Financial analysis is strong, undertaken frequently and identified performance at a practice level which enables more targeting of resources.
The MMG has a robust, systematic
The MMG holds robust discussions when
and transparent process for decision-
making decisions about the introduction of new
making as part of its overall
governance framework.
Page 21 of 70 - Primary Care Prescribing - Hywel Dda Health Board
Medicines Management Group (MMG)
Expected practice
In place?
Further information
All prescribing decisions take into
The principle that hospital contract prices are
account the impact of loss leaders in
not used (because of loss leading effects in
secondary care on primary care.
primary care) has been in place since before 2009. The Health Board uses hospital prices when the item requested will only be prescribed and supplied in secondary care. The Health Board uses STEPS (Safety, Tolerability, Effectiveness, Price, and Simplicity) which helps to focus on the most important aspects of new drugs when considering their appropriate place in therapy. This takes into consideration price in the sector where the new drug will be used.
The MMG decisions are
All MMG decisions are communicated via a
communicated in a timely way.
report to the Quality and Safety Committee which ratifies the decisions. Once agreed they are incorporated into the Health Board's Prescribing Newsletter and circulate to all internal staff via the global email system and externally to GP practices and Community Pharmacists across the Health Board via email and post. The formulary and GP ScriptSwitch systems are also updated. We found no evidence that these arrangements are not working.
Interface working between primary and secondary care
Expected practice
In place?
Further information
There is a policy or working protocols
Since our review of interface prescribing in
which ensures safe transfer of
2010, the Health Board has made
medicines and information across the
improvements to the quality of shared care
primary care secondary care
protocols (SCP). SCPs are developed with
consultant and GP engagement and are available on the intranet. The requirement for a new SCP is linked to the formulary risk assessment. One new SCP has been developed for mycophenolate in rheumatology. The Health Board did try to develop a SCP for ADHD but constraints relating to the GMS contract were a barrier.
Monitoring of the use of SCPs by GPs is via the post payment verification visits.
Page 22 of 70 - Primary Care Prescribing - Hywel Dda Health Board
Interface working between primary and secondary care
Expected practice
In place?
Further information
The Health Board has medicines
reconciliation arrangements in place
/ The Health Board's risk register has a red risk
of ‘Patients receiving wrong medication &
on admission to hospital which
delays in treatment by GP's who have
identifies the most accurate list of a
inadequate information." Mitigation is primarily
patient's medicines and will enable
with the national work led by NWIS.
any discrepancies to be recognised
The Health Board needs to meet the 90 per
and changes documented, thereby
cent target for receiving medicines
resulting in a complete list of
reconciliation review in the first 24 hours
medications that the patient is being
following admission. Audits show a high level
of compliance and the Health Board is aware that higher levels would only be possible with more capacity and seven day working.
Timely discharge letters are sent to
GPs, containing clear and relevant
/ Discharge letters remain a significant issue for
the Health Board. To take out prescriptions
information to help support
(TTOs) are not well completed and can be
prescribing decisions in primary care.
poorly written and illegible leading to the
potential for prescribing errors which may
identify that the patient's condition
subsequently harm patients or lead to
readmission to hospital. This issue was raised
contain the reasons for any
in our 2010 Interface Prescribing report.
medication change;
The Health Board supports and monitors a
identify recommended medicines
Discharge Medicines Review Service (DMR)
by generic name and therapeutic
with community pharmacies to improve patient
care after leaving hospital by allowing
pharmacists to check prescriptions to ensure
give the reason why any branded
that the right medication has been prescribed
medicines are recommended; and
and in the correct dosage. The Health Board
give the reason why unlicensed or
has recently undertaken a pilot to move from
off label drugs are recommended.
handwritten prescriptions for surgical patients to using the Myrddin patient administration system. This has shown positive results and areas to develop before rolling it out to other wards. This is a welcome innovation which should provide benefits for patient safety and reductions in staff time once it is fully implemented across the Health Board.
Page 23 of 70 - Primary Care Prescribing - Hywel Dda Health Board
3. Delivering safe, effective and economical prescribing
13. The Health Board has set realistic budgets and achieved financial savings from the
primary care prescribing budget and can make further progress to support the safety, quality and economy of local prescribing. We have come to this conclusion because:
Budget setting and financial performance: the target set for savings from
primary care prescribing was £4.3 million in 2012-13 which was achieved at year
end. The Health Board sets its annual prescribing budgets based on historic
expenditure, growth and cost pressures. Detailed information on meeting
financial targets is prepared monthly and scrutinised by the MMG.
Overall expenditure on primary care prescribing: the Health Board currently
spends £65 million on primary care drugs and the spend is similar to the average
for Wales when adjusted to take into consideration the numbers of older people
in the population.
Indicators of effective prescribing: the Health Board has low levels of generic
prescribing and high levels of prescribing on preparations not recommended by
NICE which indicate that, by targeting these and other areas highlighted in this
section, the Health Board could make additional annual savings of around
£2.1 million without affecting patient care.
Prescribing on wound management, food supplements and incontinence
products: while the Health Board has been successfully targeting wound
management and food supplements, there are still savings to be made by
improving prescribing of these products.
National prescribing indicators (NPIs): the Health Board performs mid-range
on most NPIs and are better than average for prescribing morphine as a
percentage of strong opioid items; but they are the worst for prescribing long
acting insulin and below average on ACE inhibitor4, proton pump inhibitor and
hypnotic and anxiolytic prescribing highlighting the need to move the focus of
prescribing support to these indicators.
Adverse drug reaction (ADR) reporting: the Health Board has low compliance
with the Yellow Card reporting of ADRs and has recently appointed a Yellow
Card champion to develop work in this area; but there are significant issues with
the Datix adverse event reporting as GPs have disengaged from the process.
Drug wastage: medicine waste is highlighted on the risk register and the Health
Board has initiated a number of activities to reduce waste and make financial
savings demonstrating its commitment to this area of work.
14. The following tables summarise the findings supporting the conclusion.
4 Angiotensin-converting enzyme (ACE) inhibitors are medicines used commonly in the treatment of high blood pressure.
Page 24 of 70 - Primary Care Prescribing - Hywel Dda Health Board
Budget setting and financial performance
Expected practice
In place?
Further information
There needs to be clear approach
The Health Board sets its annual prescribing
to primary care prescribing budget
budgets based on historic expenditure, growth
and cost pressures. Detailed work is
is fair and adequate to meet the
undertaken and the budget setting process is
clinical needs of patients;
open and transparent.
takes into account increases in
prescribing that will be required for improvements in the clinical aspects of prescribing;
takes into account
improvements in the cost-effectiveness of prescribing that need to be made; and
uses an open and transparent
Expenditure on primary care
The target set for savings from primary care
prescribing remains within budget
prescribing was £4.3 million in 2012-13. This
and savings targets are attained.
target was achieved at year end.
Financial monitoring takes place at
The team monitors expenditure based on the
team level and action is taken if
methodology used at Cwm Taf Health Board.
targets are not being met.
While GPs who are not meeting their targets will get less from the prescribing management scheme, they are also targeted for additional support.
Financial monitoring takes place at
The prescribing team produce a prescribing
report on a monthly basis setting out detailed information on prescribing expenditure and an explanation of the risks that could affect meeting the savings target. This is monitored closely by the prescribing work stream. The MMG has executive board level representation and is provided with updates from the Director of Finance.
Page 25 of 70 - Primary Care Prescribing - Hywel Dda Health Board
Overall expenditure on primary care prescribing
Expected practice
In place?
Further information
The reasons for the current Health
The Health Board spent £65 million on primary
Board expenditure on primary care
care drugs June 2012 and May 2013.
prescribing are known and
Appendix 2 sets out the expenditure by the 15
British National Formulary (BNF) chapter headings adjusted per population prescribing unit which takes into consideration the numbers of older people in the population. The adjusted spend in Hywel Dda was £115,458 per 1,000 prescribing units (PUs) which is similar to the average for Wales.
15. The tables below summarise how the Health Board is performing against a range of
prescribing indicators reviewed as part of the audit. Additional graphical comparisons are provided in Appendix 3 of the report.
Indicators of effective prescribing
Expected practice
Health Board's performance
The Health Board can generate further
We estimate that the Health Board could make
savings by matching overall prescribing to
additional annual savings of around £2.1 million
that achieved within the best quartile of GP
without affecting patient care (see Appendix 1 for
The Health Board has high levels of generic
Appendix 3: Exhibit 1 shows that the Health Board
prescribing matching best GP quartile
could potentially realise £473,000 by improving
performance (85 per cent) which reflects high
generic prescribing.
quality prescribing such as lower error rates and costs. To reduce the impact of variation a basket of commonly prescribed drugs with generic equivalents has been developed (Appendix 3: Exhibit 2) to identify realisable savings by improving generic prescribing.
Page 26 of 70 - Primary Care Prescribing - Hywel Dda Health Board
Indicators of effective prescribing
Expected practice
Health Board's performance
The BNF describes a number of drugs which
The Health Board spent over £56,000 on
are less suitable for prescribing because they
preparations that are less suitable for prescribing
have limited clinical value, they have been
between March and May 2013 (Appendix 3: Exhibit
superseded by more effective drugs or they
3). This suggests the Health Board has both quality
have significant side effects.
and savings opportunities of around £112,000 over
If 50 per cent of prescriptions on these
preparations were discontinued then the Health Board could realise savings.
NICE has identified a number of drugs not
The Health Board spent £18,000 on drugs not
recommended for routine use. Performance
recommended for routine use (Appendix 3:
against a basket of drugs5 in this category
Exhibit 4). This suggests that focused prescribing
reflects effective and safe within primary care
advice could provide £36,000 savings.
Prescribing on wound management, food supplements and incontinence products
Expected practice
Health Board's performance
Antimicrobial dressings
Appendix 3: Exhibit 5 shows that between
While antimicrobial dressings are widely used September 2011 and August 2012 the Health Board evidence for their use in primary care is
spent £1.6 million on wound dressings and has a
limited and of poor quality. In view of the
high percentage of prescribing on antimicrobial
multitude of dressings available, the absence
of specific advice in national guidelines, and
The Health Board has developed a wound
recognising financial constraints, local
formulary for GPs which has achieved significant
formularies provide a means of rationalising
savings of £340,000 which is a 15 per cent saving
choice of dressings.
over three years. Engagement with District Nurses
The Health Board could realise savings by
has been seen as a key strength of this work,
moving all GPs towards the levels of
supported by accountability for ordering and
antimicrobial wound dressings prescribed to
engagement of a Tissue Viability Nurse to
the best performing Health Board.
demonstrate the clinical efficacy of the chosen products on the formulary. This approach demonstrates good practice and is to be commended. However, prescribing of anti-microbial dressings is still higher than the Wales average so there is the potential to realise savings of £36,000 if they matched the proportion of antimicrobial wound dressings prescribed to the best performing Health Board.
5 This basket comprised Aliskiren, Cilostazol, Roflumilast, Linagliptin, Paricalcitol, and Hyaluronic Acid (Sodium).
Page 27 of 70 - Primary Care Prescribing - Hywel Dda Health Board
Prescribing on wound management, food supplements and incontinence products
Expected practice
Health Board's performance
Food supplements
Appendix 3: Exhibit 6 shows that between March
The evidence base for oral nutritional
2013 and May 2013 the Health Board spent over
supplements was assessed by the NICE.
£297,000 on food supplements (sip feeds) at an
This review concluded that until further
average cost of £38.23 per item which is the lowest
evidence is available, people with weight loss
in Wales. Therefore we have not suggested any
secondary to illness should either be
additional savings from reducing the cost per item.
managed by referral to a dietician, or by staff
The Prescribing Support Dietician has developed a
using protocols drawn up by dieticians, with
formulary for SIP feeds based on the currently
referral as necessary. Evidence gained
prescribed list. They plan to refine this list and work
during the Wales Audit Office hospital
to reduce inappropriate prescribing.
catering study suggested nutritional
supplements are poorly managed in the community; costs are high as is wastage.
If the item cost were reduced to the lowest average cost in Wales the Health Board could release savings. Further savings may be forthcoming if the quantity of items is reduced
Incontinence and stoma products
Appendix 3: Exhibit 7 shows that the Health Board
A 2010 national audit of incontinence found
spent over £2.3 million on stoma appliances and
the great majority of continence services are
around £372,000 on incontinence appliances. The
poorly integrated across acute, medical,
level of prescribing per 1,000 PUs for both types of
surgical, primary, care home and community
product suggests that some quality and savings
settings, resulting in disjointed care for
improvements could be found by targeting this area.
patients and carers. In primary care
Pembrokeshire GPs have had approval to recruit a
incontinence and stoma appliances are
stoma nurse with the monies they have saved on
usually provided to patients by a prescription
the prescribing management scheme which should
written by their GP or a nurse prescriber. This help deliver improvements. prescription is then dispensed by one of the following a dispensing appliance contractor, a pharmacy contractor or a dispensing doctor. A focused approach to improve quality and quantity of prescribing incontinence and stoma products can realise cost savings.
Page 28 of 70 - Primary Care Prescribing - Hywel Dda Health Board
Performance against the national prescribing indicators 2011-12
Expected practice
Health Board's performance
ACE inhibitor
Appendix 3: Exhibit 8 shows that the Health Board
ACE inhibitors (angiotensin-converting
prescribing of ACE inhibitors could be improved as
enzyme inhibitors) are medicines used
it is the second lowest in Wales at 73.12 per cent. If
commonly in the treatment of high blood
the Health Board achieved the levels of the best
pressure. NICE Clinical Guidelines (CG34)
performing GP quartile, savings would amount to
states that the benefit from ACE inhibitors
over £116,000 (Appendix 3: Exhibit 9).
and angiotensin-II receptor antagonists were
closely correlated although due to cost differences, ACE inhibitors should be initiated first.
Matching the best performing GP quartile would potentially realise savings.
Proton pump inhibitors (PPIs)
Appendix 3: Exhibit 10 shows that Hywel Dda's rate
PPIs are used for the treatment of
of prescribing the least expensive PPIs is low at
oesophageal reflux disease, dyspepsia, or
93.67 per cent. Increasing the use of low acquisition
gastric ulcers. Although concerns are now
cost PPIs provides the Health Board with potential
being expressed about the safety of long
savings, and if performance matched the best GP
term prescribing of PPIs, NICE
quartile, they would amount to over £128,000
recommendations state that the least
(Appendix 3: Exhibit 11).
expensive PPI should be used.
Matching the best performing GP quartile (96.61 per cent) would potentially realise savings.
Performance against the national prescribing indicators 2012-13
Expected practice
Health Board's performance
Ibuprofen and naproxen non-steroidal
Appendix 3: Exhibit 12 shows that, the Health
anti-inflammatory drugs (NSAIDs)
Board is performing well although at 74.05 per cent
NSAIDs are medications widely used to
the level of prescribing still falls below the national
relieve pain, reduce inflammation and reduce
target level. This performance suggests more could
fever. There is overwhelming evidence to
be done to improve the quality of prescribing.
reduce prescribing of NSAIDs especially for
Appendix 3: Exhibit 13 shows that and increasing
the elderly. If NSAIDs have to be prescribed,
the use of ibuprofen and naproxen will also provide
to reduce risk ibuprofen and naproxen are
the Health Board with potential savings of £49,000
accepted as the first line choice.
if they achieved the best GP quartile prescribing
Matching the best performing GP quartile
(79.63 per cent) would potentially realise savings.
Page 29 of 70 - Primary Care Prescribing - Hywel Dda Health Board
Performance against the national prescribing indicators 2012-13
Expected practice
Health Board's performance
Low acquisition cost statins
Appendix 3: Exhibit 14 shows that the Health
Current NICE guidelines promote the use of
Board's rate of prescribing low acquisition statins is
low acquisition statins as first-line treatment
93.80 per cent against a target of 95 per cent. If the
for most people with established
Health Board achieved the best GP quartile
atherosclerotic vascular disease, those with
performance this would not only deliver better
diabetes and others with a high risk of
outcomes it would also deliver an additional
cardiovascular disease (CVD). This has been
£342,000 saving (Appendix 3: Exhibit 15).
found to be the most cost-effective
Matching the best performing GP quartile (96.26 per cent) would potentially realise savings.
Long acting insulin for type 2 diabetes
Appendix 3: Exhibits 16 shows that the Health
NICE guidance on the management of type 2
Board is above target and has the highest
diabetes recommends that when insulin
prescribing rate for long acting insulin of all the
therapy is necessary, human isophane (NPH) health boards (95.67 per cent). Potential savings of insulin is the preferred option. Long-acting
£36,000 could be achieved if the Health Board
insulin analogues have a role in some
achieved the best GP quartile (Appendix 3: Exhibit
patients, and can be considered for those
who fall into specific categories. However, for
most people with type 2 diabetes, long-acting
insulin analogues offer no significant advantage over human NPH insulin, and are much more expensive. Matching the best performing GP quartile (87.88 per cent) would potentially realise savings.
Opioids for pain relief
Appendix 3: Exhibit 18 shows that at 48.77 per cent
Opioids have a well-established role in the
the Health Board has the second highest level of
management of acute pain following trauma
morphine prescribing as a percentage of strong
(including surgery), and in the management
opioid items in Wales. Although this is a relatively
of pain associated with terminal illness.
good performance it still falls below the target of
Morphine remains the most valuable opioid
50.60 per cent. If the Health Board could match the
analgesic for severe pain.
best performing GP quartile, it has the potential to
Matching the best performing GP quartile
release over £224,000 in savings (Appendix 3:
(55.93 per cent) would potentially realise
Page 30 of 70 - Primary Care Prescribing - Hywel Dda Health Board
Performance against the national prescribing indicators 2012-13
Expected practice
Health Board's performance
Antibacterial prescribing – top nine items
Appendix 3: Exhibit 20 shows that the Health
The Health Protection Agency guidance for
Board's prescribing of the top nine antibacterials is
primary care identifies the most appropriate
81.46 per cent which is below the target rate of
treatment protocol and antibiotics for
common infections experienced in primary
care. The top nine antibacterials provide sufficient cover to treat upper and lower respiratory tract infections, urinary tract infections (UTIs) and common skin infections.
The use of simple generic antibiotics and the avoidance of broad-spectrum reduce the risk resistant bacteria pose now and for the future.
Target is 83.58 per cent for top nine antibacterials as a percentage of antibacterial items.
Antibacterial prescribing – overall
The overall prescribing rate for antibacterial items in
prescribing rate
the Health Board is high at 351.41items per 1,000
Antimicrobial Resistance Programme in
STAR-PUs (Appendix 3: Exhibit 21). This
Wales supports and promotes the prudent
performance suggests there is scope for reducing
use of antimicrobials.
the use of antibacterials.
The development of a structured programme to reduce antibiotic prescribing by GPs could minimise the potential for antibiotic resistance developing locally. Target is 329 items per 1,000 STAR-PUs.
Page 31 of 70 - Primary Care Prescribing - Hywel Dda Health Board
Performance against the national prescribing indicators 2012-13
Expected practice
Health Board's performance
Broad spectrum antibiotics
Primary care prescribers in the Health Board are using high levels of the broad spectrum antibiotics.
There is an association between quinolone
Appendix 3: Exhibits 22-24 show that prescribing of
use and the incidence of C. difficile
co-amoxiclav is particularly high and the Health
associated diarrhoea therefore, use should
Board has the second highest rate of prescribing of
be restricted to specific indications in order to
these antibiotics in Wales.
reduce the risk of potential antimicrobial resistance. The average cost of a C. difficile
Reducing the rate of these three antibiotics is a
infection has been estimated to be £4,007
feature of the 2013-14 NPIs because of the risk of
which shows there are whole system and
antiobiotic resistance developing. Prescribing
potential long term consequences of not
performance suggests there is significant scope to
managing quinolone prescribing.
improve the quality of prescribing in this area. The Health Board is recruiting a specialist antimicrobial
The cephalosporins are broad-spectrum
pharmacist which should support this area of work
antibiotics which are used for the treatment of across the Health Board.
septicaemia, pneumonia, meningitis, biliary-tract infections, peritonitis, and UTIs.
The use of broad spectrum antibiotics should be restricted to specific indications in order to reduce the risk of antimicrobial resistance.
Targets have been set as a percentage of all antibacterials prescribed: cephalosporins 3.14 per cent; co-amoxiclav 2.99 per cent; and quinolones 1.42 per cent.
Dosulepin
The Health Board's prescribing of dosulepin is
Dosulepin is an antidepressant, historically
lower than some other Health Boards at 66.70 DDD
used where an anti-anxiety or sedative effect
per 1000 PUs (Appendix 3: Exhibit 25) but is still
is required; however it does have a small
well above target of 52.15. Appendix 3: Exhibit 27
margin of safety between the maximum
shows that many GPs are continuing to prescribe
therapeutic dose and a potentially fatal dose.
high levels of dosulepin and will need support to
Current NICE guidance is not to switch to, or
work with patients to reduce the use of this
start, dosulepin because evidence supporting
medication. To meet NICE guidance the medicines
its tolerability relative to other
management team should target this area for
antidepressants is outweighed by the
reduction jointly with mental health staff.
increased cardiac risk and toxicity in
overdose. A focused approach to reduce prescribing of dosulepin should improve the quality of care and reduce the risk to patients. Target is 52.15 DDD per 1000 PUs6.
6 Defined daily dosage (DDD) of Dosulepin Hydrochloride per 1,000 PUs.
Page 32 of 70 - Primary Care Prescribing - Hywel Dda Health Board
Performance against the national prescribing indicators 2012-13
Expected practice
Health Board's performance
Hypnotics and anxiolytics
Appendix 3: Exhibit 26 shows that the Health Board
There has been concern over the high
has high rates of prescribing of hypnotics and
volume of anxiolytic and hypnotic prescribing
anxiolytics (2014.12 DDD per 1,000 patients). Many
within Wales. It is recognised that some
GPs are prescribing above target, some
prescribing may be inappropriate and
significantly so.
contribute to the problem of addiction and
Our audit found that the Ceredigion prescribing
masking underlying depression. There are
team has provided support to GPs to reduce use of
also whole system consequences of the
hypnotics through providing patients with resources
additional costs of providing addiction
for self-help. The GPs have had some success but
services to manage dependency.
they need a lot of support to keep people off these
A focused approach to reduce prescribing of
drugs. There is no mental health representative on
hypnotics and anxiolytics should improve the
the MMG although one is being sought. Further
quality of care and reduce the risk to patients. support is needed to develop work with mental Target 1402 DDD per 1000 PUs.
health teams to provide counselling and other support to provide alternatives to medication for people with anxiety and depression.
Page 33 of 70 - Primary Care Prescribing - Hywel Dda Health Board
Adverse drug reaction (ADR) monitoring
Expected practice
In place?
Further information
The Yellow Card Scheme is run by
The medicines management and pharmacy
the Medicines and Healthcare
/ strategy contains an aim to improve patient
products Regulatory Agency
safety via the following actions:
(MHRA) and the Commission on
to increase the level of yellow card reporting;
Human Medicines (CHM), and is
share information on incidents;
used to collect information from
implement NPSA patient alerts; and
both healthcare professionals and
the general public on suspected
ensure learning takes place from Datix
side effects or adverse drug
reaction ADRs to a medicine. This
While it is positive to see that the Health Board
scheme is vital in helping the
recognises the need to improve patient safety
MHRA monitor the safety of the
there is a low level of incident reporting and this
medicines and vaccines that are on
performance is continuing to worsen (Appendix
4: Exhibits 30-32).
The 1998 Audit Commission work
The Health Board implemented Datix across the
highlighted low levels of reporting of
Health Board and in GP practices to collect
ADRs in Wales and this trend has
information about safety incidents. But GPs told
not improved AWMSG has agreed
us of their difficulties using Datix and that even
that Yellow Card reporting would be
when they did use the system no action was
used as a local comparator across
taken on their concerns. GPs are continuing to
Wales. Alongside this YCC Wales
use their own serious incident reporting
has developed an education
mechanisms but these do not link to the Health
programme which is available to
Board. This is an issue that the Health Board
GPs and health boards.
needs to resolve.
Good practice for ADR prevention
As set out in our prescribing interface review in
and reporting is set out in
2010, issues remain with capturing incidents
Appendix 4: Exhibit 34.
from local community pharmacies. Community pharmacies do not use Datix and incident
reporting does not form part of the community pharmacy contract. The Health Board relies on the completion of incident proformas, and there is no formal monitoring of this.
The Multidisciplinary Medication Event Review Group (MERG) aims to review all reported errors and near misses involving medication, which includes prescribing, preparation, dispensing and administration of medication; the aim being to prevent similar near misses/errors reoccurring. This group was meeting infrequently, due to a lack of engagement from clinicians although it has now met and is drawing up its work plan.
Page 34 of 70 - Primary Care Prescribing - Hywel Dda Health Board
Adverse drug reaction (ADR) monitoring
Expected practice
In place?
Further information
The MMG provides the Health Board's Quality and Safety Committee with a report updating them on the decisions and key issues arising from meetings. This report does not cover monitoring of ADRs or patient safety incidents.
The Medicines Management team recently appointed a yellow card champion to lead on this agenda. She has now, created links with hospital pharmacy departments and completed initial training programme.
Drug wastage
Expected practice
In place?
Further information
The Welsh Government has
estimated that the cost of wasted
/ Assuming the levels are consistent across
Wales, we estimate that the cost of wasted
drugs amounts £50 million each
drugs is £6.4 million. If the Health Board could
reduce this by 50 per cent up to £3.2 million
The Health Board could reduce
could be saved (Appendix 5: Exhibit 34).
wastage by up to 50 per cent.
The Health Board has information
Medicine waste is highlighted on the risk register
on medicine wastage levels for
and the Health Board has estimated the financial
example audits have been
impact associated with wastage is £1.5 million,
although the source of this figure was unclear. They should undertake an audit to establish the scale of wastage across the counties and then develop appropriate strategies based on this information.
The Health Board is using the
The Health Board is using community
community pharmacy contract to
pharmacies to participate in the awareness
reduce wastage for example
raising with the public and delivering its
incentivising management of
campaign. Discharge Medicines Reviews (DMR)
medicines at the start of
and Medicines Use Reviews (MUR) are in place
and while they have got off to a slow start they are gaining momentum. Information on the DMRs was contained in the prescribing newsletter to raise awareness of prescribers of the service and what it offers. However, GPs raised concerns that DMRs can be an issue, as community pharmacists are contacting GPs for information and this is causing extra workload.
Page 35 of 70 - Primary Care Prescribing - Hywel Dda Health Board
Drug wastage
Expected practice
In place?
Further information
Some issues with repeat dispensing schemes and governance arrangements with breaches of the standard operating procedures (SOP) were reported. In order to remedy the problem the pharmacists have issued guidance to community pharmacies. This is an area for further development.
While one of the main reasons for
The Health Board risk register highlights the
returning medicines is the death of
issue of drug wastage, and mitigating actions
the patient, recent work has
are defined, but not all policies are delivering
identified the following processes
and systems cause medicines to be
Addressing the wastage of drugs is a clear
priority for the Health Board. They are
complex treatment regimens
participating in a public campaign with other
leading to patients not following
Health Boards. Launched in early 2013, this
or completing the treatment;
campaign has identified that Hywel Dda wastes
changing treatments and
£2.7 million on medications, and wants patients
unnecessary switching between
to order only what they need; return unwanted
medications and bring medications into hospital
long prescription durations –
when they are being treated as inpatients. A
limiting to 28 days is the most
similar campaign in 2009 realised savings of
cost effective regimen reducing
£145,000. Based on the previous campaign it is
returns to pharmacies;
anticipated they can reduce the number of items
dispensed by 0.25-0.5 per cent. It is too early to
repeat prescribing and
evaluate the results of this.
dispensing processes leading to over supply;
lack of appropriate medicine use
support in the home; and
lifestyle and events which
disrupt medicine taking routines.
Page 36 of 70 - Primary Care Prescribing - Hywel Dda Health Board
Summary of potential savings This appendix provides further information on the comparative performance of the Health Board against a range of prescribing indicators, and potential savings that have been identified from these comparisons. The table below summarises the basis of the savings calculations that have been used.
This appendix provides further information on the comparative performance of the Health Board against a range of prescribing indicators, and potential savings that have been identified from these comparisons. The table below summarises the basis of the savings calculations that have been used.
Indicator
Basis of savings calculation used in this report
The best quartile of GP practices in Wales realise 85 per cent levels of generic prescribing. Some branded drugs (such as Ventolin and Zapain) which are prescribed in large quantities and are currently cheaper than generic equivalents. Depending on case mix individual GP practices may have more or less potential to realise savings in this area.
To reduce the impact of variation a basket of commonly prescribed
Generic prescribing
drugs with generic equivalents has been developed to identify realisable savings by improving generic prescribing.
Savings have been calculated for each of a basket of proprietary drugs by taking the actual expenditure on proprietary drugs (March 13 - May 13) minus the costs of the generic alternative (based on 21 August 2013 prices in the BNF) and then multiply the savings by four to get potential savings over 12 months, rounded to nearest 1,000.
Actual expenditure (March 13 - May 13), has been multiplied by four
Drugs identified as less
to get 12 months expenditure. Potential savings have been calculated
suitable for prescribing
by reducing the total expenditure by 50 per cent, recognising the
excluding glucosamine
sustained effort and education programme that may be required to change individual prescribers' habits.
Actual expenditure (March 13 - May 13), has been multiplied by four to get 12 months expenditure. Potential savings have been calculated
NICE non recommended
by reducing the total expenditure by 50 per cent, recognising the
sustained effort and education programme that may be required to change individual prescribers' habits.
The savings have been calculated on reducing the percentage
Antimicrobial wound dressing prescribing of antimicrobial dressings used in primary care down to
the best performing health board.
Food supplements (Sip
The savings have been calculated based on reducing current
expenditure down to the best health board average cost per item.
National prescribing
The savings have been calculated on health boards achieving the
best quartile GP practice performance.
Page 37 of 70 - Primary Care Prescribing - Hywel Dda Health Board
Summary of potential savings
Improved generic prescribing
Drugs less suitable for prescribing
NICE non recommended drug basket
Wound management and food supplements
Antimicrobial wound dressing
Food supplements
National prescribing indicators
Improved ACE inhibitor prescribing
Proton pump inhibitors
Low acquisition statins
Long acting insulin
Opioid prescribing
£1,552,000
Source: Wales Audit Office analysis of CASPA.Net data
Page 38 of 70 - Primary Care Prescribing - Hywel Dda Health Board
Comparative analysis of British National Formulary (BNF) chapter prescribing by health board
Total expenditure by BNF chapter per 1,000 Prescribing Units7 – June 2012 to May 2013
Abertawe
Cardiff and
Hywel Dda
Bro Morg-
Cadwaladr
Teaching
annwg Uni
7 Prescribing Units (PUs) take account of the greater need of elderly patients for medication in reporting prescribing performance at both the practice and health authority level. Rather than compare the cost of prescribing or the number of items prescribed by patient, comparisons by PUs would weigh the result according to the number of elderly patients in either the practice or health board. Patients aged 65 and over are counted as three PUs and patients under 65 and temporary residents are counted as one.
Page 39 of 70 - Primary Care Prescribing - Hywel Dda Health Board
Abertawe
Cardiff and
Hywel Dda
Bro Morg-
Cadwaladr
Teaching
annwg Uni
Total spend
primary care
drugs per
Source: Wales Audit Office analysis of CASPA.net8 data
8 Comparative Analysis System for Prescribing Audit.
Page 40 of 70 - Primary Care Prescribing - Hywel Dda Health Board
Analysis of prescribing indicators
Exhibit 1: Potential savings from generics based on a basket of proprietary drugs March 2013 - May 2013
Health Board
Total expenditure
Potential savings
(Mar 13 - May 13)
pro-rated for 12
months
Abertawe Bro Morgannwg
Cardiff And Vale
Source: Wales Audit Office analysis of CASPA.net
Exhibit 2: Generic drug basket
Proprietary drug
Actonel_Once A Week Tab 35mg
Imigran 50_Tab 50mg, 100mg
Actos_Tab 15mg, 30mg, 45mg
Innovace_Tab 2.5mg, 5mg,10mg,20mg
Alphagan_Eye Dps 0.2%
Istin_Tab 5mg, 10mg
Risperdal_Tab 1mg, 2mg, 3mg, 4mg
Aricept_Tab 10mg, 5mg
Lescol_Cap 20mg, 40mg
Risperdal_Tab 500mcg, 6mg
Arimidex_Tab 1mg
Lipantil Micro 200_Cap 200mg
Seroquel_Tab 25mg, 100mg, 150mg, 200mg,300mg
Bonviva_Tab 150mg F/c
Lipantil Micro 267_Cap 267mg
Seroxat_Tab 20mg, 30mg
Cardura_Tab 1mg, 2mg
Lipitor_Tab 10mg, 20mg,40mg,80mg
Subutex_Tab Subling 2mg, 8mg
Casodex_Tab 50mg,150mg
Losec_Cap E/c 10mg, 20mg, 40mg
Telfast 120_Tab 120mg, 180mg
Cipramil_Tab 10mg,20mg,40mg
Lustral_Tab 50mg,100mg
Tritace_Tab 1.25mg, 2.5 mg,5mg,10mg
Colofac_Tab 135mg
Lustral_Tab 50mg
Trusopt_Ocumeter Plus Ophth Soln 2%
Cosopt_Ocumeter Plus Eye Dps
Mirapexin_Tab 0.7mg
Tylex_Cap 30mg/500mg
Cozaar Half Strength_Tab 12.5mg,
Motilium_Tab 10mg
Xalacom_Eye Dps 50mcg/5ml/ml
25mg, 50mg, 100mg
Desmotabs_Tab 0.2mg
Naramig_Tab 2.5mg
Xalatan_Eye Dps 50mcg/ml
Page 41 of 70 - Primary Care Prescribing - Hywel Dda Health Board
Detrusitol_Tab 2mg
Neoclarityn_Tab 5mg
Zestril_Tab 5mg, 10mg,20mg,40mg,80mg
Neurontin_Cap 100mg, 300mg, 400mg,
Femara_Tab 2.5mg
Nexium_Tab 20mg, 40mg
Zyprexa_Tab 2.5mg, 5mg, 7.5mg, 10mg, 20mg
Fosamax_Once Weekly Tab 70mg
Zyprexa_Velotab 5mg,10mg, 15mg, 20mg
Source: Wales Audit Office analysis of CASPA.net
Exhibit 3: Basket of drugs identified as less suitable for prescribing (excluding glucosamine) March 2013 – May 2013 (pro-rated to 12 months)
Health Board
Total expenditure
Potential savings
(Mar 13 - May 13)
pro-rated for 12
months
Abertawe Bro Morgannwg
Cardiff and Vale
Drugs and preparations included in analysis: Simeticone, Infacol, Dentinox Infant Colic Dps'Atropine Sulphate,
Adsorbents And Bulk-Forming Drugs, Codeine Phosphate Compound Mixtures'Co-Phenotrope (Diphenox
HCl/Atrop Sulph), Opium & Morphine, Loperamide Hydrochloride & Dimeticone, Liquid Paraffin, Liq Paraf & Mag
Hydrox_Oral Emuls, Rowachol, Co-Flumactone (Hydroflumeth/Spironol), Spironolactone With Thiazides, Diuretics
With Potassium Clonidine Hydrochloride, Guanethidine Monosulphate, Trandolapril + Calcium Channel Blocker,
Cinnarizine, Calcium Dobesilate, Nicotinic Acid Derivatives, Pentoxifylline, Rutosides, Moxisylyte Hydorchloride,
Cerebral Vasodilators, Etamsylate, Ephedrine Hydrochloride, Cough Preparation, Systemic Nasal Decongestants,
Cloral Betaine, Meprobamate, Promazine Hydrochloride, Gppe Tab_Triptafen, Gppe Tab_Triptafen-M, Triptafen,
Clomipramine Hcl_Tab 75mg M/r, Anafranil, Dosulepin Hydrochloride, Isocarboxazid, Tranylcypromine Sulphate,
Dexfenfluramine Hydrochloride, Diethylpropion Hydrochloride, Fenfluramine Hydrochloride, Mazindol, Phentermine,
Rimonabant, Metoclopramide Hcl_Tab 15mg M/r, Metoclopramide Hcl_Cap 30mg M/r, Metoclopramide Hcl_Cap
15mg M/r, Maxolon Sr_Cap 15mg, Co-Codaprin, Papaveretum, Pentazocine Hydrochloride, Pentazocine Lactate,
Pamergan, Migraleve, Ergotamine Tartrate, Midrid, Clonidine Hydrochloride, Methysergide, Minocycline
Hydrochloride, Methenamine Hippurate, Methenamine Hippurate, Inosine Pranobex, Stavudine, Indinavir,
Pyrimethamine, Hydrocortisone Sodium Phosphate, Bethanechol Chloride, Rowatinex_Cap, Ferrograd, Feospan,
Ferrograd, Slow-Fe, Ferrograd-Folic, Cyanocobalamin, Slow-K, Cyanocobalamin (b12), Vit B Co_Tab, Vit B,
Co_Syr, Vit B Comp_Cap, Vit B Comp_Tab, Potaba_Cap 500mg, Potaba_Envules 3g, Potaba_Tab, Bitters And
Tonics, Icaps_Tab, Icaps Oad_Tab, Icaps Plus_Tab, Piroxicam, Methocarbamol, Kaolin Heavy, Freeze Sprays &
Page 42 of 70 - Primary Care Prescribing - Hywel Dda Health Board
Gels, Docusate Sodium, Cerumol, Isopropyl Alcohol, Urea Hydrogen Peroxide, Other Preparations, Ephedrine
Hydrochloride, Borax, Glucose/Glycerol, Ipratropium Bromide, Phenylephrine Hydrochloride, Xylometazoline
Hydrochloride, Fusafungine, Lozenges & Sprays, Tetracaine Hydrochloride, Benzocaine, Antazoline Hydrochloride,
Calamine, Diphenhydramine Hydrochloride, Ethyl Chloride, Mepyramine Maleate, Lidocaine, Lidocaine
Hydrochloride, Aluminium Oxide, Neomycin Sulph_Crm 0.5 per cent, Salicylic Acid, Idoxuridine In Dimethyl
Sulfoxide, Benzyl Benzoate, Permethrin_Creme Rinse 1 per cent, Permethrin_Creme Rinse 1 per cent,
Lyclear_Creme Rinse 1 per cent, Topical Circulatory Preparations
Source: Wales Audit Office Analysis of CASPA.net
Exhibit 4: NICE Basket of non-recommended drugs March 2013 – May 2013 (expenditure and savings pro-rated to 12 months)
Health Board
Total expenditure
Potentials savings pro-
(Mar 13-May 13)
rated for 12 months
Abertawe Bro Morgannwg
Cardiff and Vale
Drugs included in analysis: Aliskiren, Cilostazol, Roflumilast, Linagliptin, Paricalcitol, Hyaluronic Acid Sodium
Source: Wales Audit Office analysis of CASPA.net
Page 43 of 70 - Primary Care Prescribing - Hywel Dda Health Board
Prescribing on wound management, food supplements and incontinence products
Exhibit 5: Antimicrobial wound dressing prescribing Sept 2011 – Aug 2012
Health Board
Total wound
Potential
dressings
wound dressings
dressings
as a per cent of all
wound dressings
Cardiff and Vale
Source: Wales Audit Office analysis of CASPA.net
Page 44 of 70 - Primary Care Prescribing - Hywel Dda Health Board
Exhibit 6: Food supplement (sip feed) prescribing March 2013 – May 2013
Health Board
Expenditure
Average cost
Potential savings
(Mar 13 –
prescribed (Mar
pro-rated for 12
13 –May 13)
Cardiff and Vale
Source: Wales Audit Office analysis of CASPA.net
Exhibit 7: Expenditure on incontinence and stoma care prescribing June 2012 – May 2013
Health Board
appliances total appliances per
appliances total appliances per
expenditure
expenditure
prescribing
prescribing
Cardiff and Vale
Source: Wales Audit Office analysis of CASPA.net
Page 45 of 70 - Primary Care Prescribing - Hywel Dda Health Board
Performance against two national prescribing indicators from 2011-12
Exhibit 8: Items of ACE inhibitors as a percentage of drugs affecting the renin-angiotensin system: March 2013- May 2013
Better performance is: Higher.
Source: Wales Audit Office analysis of CASPA.net
Exhibit 9: Potential annual savings from improved ACE inhibitor prescribing
Health Board
Potential savings if LHB
achieved the best GP
quartile (79.46 per cent)
Abertawe Bro Morgannwg
Cardiff and Vale
Source: Wales Audit Office analysis of CASPA.net
Page 46 of 70 - Primary Care Prescribing - Hywel Dda Health Board
Exhibit 10: Proton pump inhibitor items of low acquisition cost as a percentage of all proton pump inhibitors: March 2013 - May 2013
Better performance is: Higher
Source: Wales Audit Office analysis of CASPA.net
Exhibit 11: Potential annual savings from improved proton pump inhibitor prescribing
Health Board
Potential savings if LHB
achieved the best GP quartile
(96.61 per cent)
Abertawe Bro Morgannwg
Cardiff and Vale
Source: Wales Audit Office Analysis of CASPA.net
Page 47 of 70 - Primary Care Prescribing - Hywel Dda Health Board
Performance against the national prescribing indicators 2012-13
Exhibit 12: Ibuprofen and naproxen as a per cent of all NSAIDs9: March 2013 - May 2013
Better performance is: Higher
Target: Maintain performance levels within the upper quartile, or show an increase towards the quartile above.
Source: Wales Audit Office Analysis of CASPA.net
9 NSAID – Non-steroidal anti-inflammatory drugs used primarily to treat inflammation, mild to moderate pain, and fever
Page 48 of 70 - Primary Care Prescribing - Hywel Dda Health Board
Exhibit 13: Potential annual savings from improved prescribing of ibuprofen and naproxen as a percentage of all NSAIDs10
Health Board
Potential savings if LHB
achieved the best GP
quartile (79.63 per cent)
Abertawe Bro Morgannwg
Cardiff and Vale
Source: Wales Audit Office analysis of CASPA.net
10Calculation of potential savings: (Difference between GP UPPER QUARTILE (3rd) and CURRENT PERFORMANCE x Non-Preferred NSAIDS AVERAGE COST PER ITEM (in 3mth reference period)) - (Difference between GP UPPER QUARTILE (3rd) and CURRENT PERFORMANCE x ibuprofen and naproxen AVERAGE COST PER ITEM (in 3mth reference period)). Potential savings were then pro-rated for one year.
Page 49 of 70 - Primary Care Prescribing - Hywel Dda Health Board
Exhibit 14: Low acquisition statin items as a percentage of all statins (including ezetimibe and ezetimibe combination products): March 2013 –May 2013
Better performance is: Higher
Target: Maintain performance levels within the upper quartile, or show an increase towards the quartile above.
Source: Wales Audit Office analysis of CASPA.net
Exhibit 15: Potential annual savings on low acquisition statins
Health Board
Potential savings if LHB
achieved the best GP
quartile 96.26 per cent
Abertawe Bro Morgannwg
Cardiff and Vale
Source: Wales Audit Office analysis of CASPA.net
Page 50 of 70 - Primary Care Prescribing - Hywel Dda Health Board
Exhibit 16: Long acting insulin items as percentage of long/interim acting insulin: March 2013 –May 2013
Better performance is: Lower Target: Maintain performance levels within the lower quartile, or show a reduction towards the quartile below
Source: Wales Audit Office Analysis of CASPA.net
Exhibit 17: Potential savings on long acting insulin prescribing
Health Board
Potential savings if LHB
achieved the best GP
quartile (87.88 per cent)
Abertawe Bro Morgannwg
Cardiff And Vale
Source: Wales Audit Office analysis of CASPA.net
Page 51 of 70 - Primary Care Prescribing - Hywel Dda Health Board
Exhibit 18: Morphine items as percentage of strong opioid items: March 2013 – May 2013
Better performance is: Higher
Target: Maintain performance levels within the upper quartile, or show an increase towards the quartile
Source: Wales Audit Office analysis of CASPA.net
Exhibit 19: Potential annual savings from improved opioid prescribing
Health Board
Potential savings if LHB
achieved the best GP
quartile (55.93 per cent)
Abertawe Bro Morgannwg
Cardiff and Vale
Source: Wales Audit Office Analysis of CASPA.net
Page 52 of 70 - Primary Care Prescribing - Hywel Dda Health Board
Exhibit 20: Top nine antibacterial as a percentage of antibacterial items: June 2012 – May 2013
Better performance is: Higher Target: Maintain performance levels within the upper quartile, or show an increase towards the quartile above.
Source: Wales Audit Office analysis of CASPA.net
Exhibit 21: Antibacterial Items per 1000 STAR- PU: March 2013 – May 2013
Better performance is: Lower Target: Maintain performance levels within the lower quartile, or show a reduction towards the quartile below
Source: Wales Audit Office analysis of CASPA.net
Page 53 of 70 - Primary Care Prescribing - Hywel Dda Health Board
Exhibit 22: Cephalosporin items as a percentage of antibacterial items by health board: June 2012 – May 2013
Better performance is: Lower Target: Maintain performance levels within the lower quartile, or show a reduction towards the quartile below
Source: Wales Audit Office analysis of CASPA.net
Exhibit 23: Quinolone items as a percentage of antibacterial items by health board: June 2012 – May 2013
Better performance is: Lower Target: Maintain performance levels within the lower quartile, or show a reduction towards the quartile below
Source: Wales Audit Office analysis of CASPA.net
Page 54 of 70 - Primary Care Prescribing - Hywel Dda Health Board
Exhibit 24: Co-amoxiclav items as a percentage of antibacterial items by health board: June 2012 – May 2013
Better performance is: Lower Target: Maintain performance levels within the lower quartile, or show a reduction towards the quartile below
Source: Wales Audit Office analysis of CASPA.net
Page 55 of 70 - Primary Care Prescribing - Hywel Dda Health Board
Exhibit 25: Dosulepin daily defined dosage (DDD) quantity per 1000 PUs: March 2013 – May 2013
Better performance is: Lower Target: Maintain performance levels within the lower quartile, or show a reduction towards the quartile below
Source: Wales Audit Office analysis of CASPA.net
Exhibit 26: Hypnotics and anxiolytics DDD quantity per 1000 patients: March 2013 – May 2013
Better performance is: Lower Target: Maintain performance levels within the lower quartile, or show a reduction towards the quartile below
Source: Wales Audit Office analysis of CASPA.net
Page 56 of 70 - Primary Care Prescribing - Hywel Dda Health Board
Reducing adverse drug reactions
Exhibit 30: Adverse drug reaction reports per 100,000 population
Source: Yellow Card Centre Wales
Exhibit 31: Decline in GP Yellow Card reporting across Wales
Source: Yellow Card Centre Wales
Page 57 of 70 - Primary Care Prescribing - Hywel Dda Health Board
Exhibit 32: ADR report sources 2011-2012
Source: Yellow Card Centre Wales
Page 58 of 70 - Primary Care Prescribing - Hywel Dda Health Board
Exhibit 33: Good practice for ADR prevention and reporting
ADR prevention and reporting
Training in primary care
Promotion of distance learning packages, for example The Wales Centre for Pharmacy Professional Education (WCPPE) packages, ADRs – Online and the MHRA e-Learning package
One to one educational visits
Individualised educational letters and follow up calls from pharmacists
Pharmacists checking prescriptions to identify errors
Medicine reconciliation on discharge and in primary care
Incentive schemes
Introduction of e-prescribing systems
Alerts and prompts on IT systems
Minimising human factors through system design, and workflow
Source: MHRA and Yellow Card Scheme
Page 59 of 70 - Primary Care Prescribing - Hywel Dda Health Board
Managing drug wastage The Welsh Government has estimated that the cost of wasted drugs amounts £50 million each year. In the absence of any detailed data available in Wales and assuming the levels are consistent across health boards the following exhibit identifies potential costs and potential savings reducing wasted medicines by 50 per cent. We have used this adjustment to address genuine reasons for drugs being wasted including the death of patient and changes in treatment.
Exhibit 34: Potential cost of wasted drugs
Health Board
Potential wastage
Potentials savings
based on 50 per cent
reduction
Abertawe Bro Morgannwg
Cardiff and Vale
Hywel Dda
£6,400,000
£3,200,000
Source: Wales Audit Office
Page 60 of 70 - Primary Care Prescribing - Hywel Dda Health Board
Primary care prescribing advice diary exercise Health boards have varying levels of primary care medicines management and prescribing support staff, largely determined by the resources they inherited from the trusts that established them. The level of resources tends to be lower in relation to population for those health boards with a smaller, and more urban, geographical area.
Health Board teams consist mainly, though not exclusively, of pharmacists and pharmacy technicians. They carry out a substantial amount of work that indirectly supports their activities within general practices, the wider community, and in relation to secondary care. The teams are a vital component in the approach to improving the quality and economy of prescribing. They should be able to target and prioritise their activities according to the performance of the practices they work with.
Health Boards use pharmacists and other support staff to help GPs improve their prescribing by:
visiting practices to support and advise GPs and other primary care staff;
developing and implementing guidance on prescribing;
analysing prescribing data, monitoring formulary compliance and providing feedback to GPs; and
undertaking projects to improve primary care prescribing, improving quality and reducing costs.
In carrying out this work it is generally accepted that the most effective approaches are:
personalised communication with GPs from local experts;
involving the whole prescribing community across primary and secondary in decisions on local drug policies; and
providing local incentives through the GMS and Community Pharmacy contracts.
As part of the audit the Wales Audit Office undertook an activity analysis of the Health Board's three County based prescribing teams. Each team member completed an activity diary over a one or two week period, depending on whether they had a full or part-time role. We grouped team activities into four categories: health board activities; working with GP practices; working in the community; and working with secondary care. It is important to remember that this exercise provides a snapshot of team activity. Team members' activities may vary from week to week, as well as through annual cycles of work. A summary of the analysis from this exercise, showing the findings for each team by each of the four categories of activity, is given Exhibit 35.
Page 61 of 70 - Primary Care Prescribing - Hywel Dda Health Board
Exhibit 35: Analysis of activity by prescribing advice teams across four main categories of work
Prescribing team
Working in
activities
practices
community
secondary
Average for the three teams
Source: Wales Audit Office analysis of prescribing team activity diary exercise
Our analysis found that on average across the three teams over half of their time is spent working on Health Board activities. The highest proportion of time in each area was spent on these activities:
health board activities – support and audit relating to the GP contract QoF and Medicines Management Local Enhanced Services; travelling time; unspecified administrative tasks; supporting the development and maintenance of the LHB formulary; preparation and analysis of CASPA data;
working with GP practices – supporting and undertaking clinical audit to identify compliance with guidance; promoting cost effective prescribing by utilising medication changes eg, switches or lower cost equivalent identified under LES 2012-13;
working in the community – supporting medication reviews within local care homes and for housebound patients; and
working with secondary care – developing shared care protocols; answering queries from GPs regarding a TTO or an OPD letter; undertaking secondary care pharmacy advisory work.
Exhibit 38 compares the findings from this exercise at each health board in Wales. This shows a similar pattern to the Welsh average.
Page 62 of 70 - Primary Care Prescribing - Hywel Dda Health Board
Exhibit 36: Analysis of Health Board prescribing advice activity
Source: Wales Audit Office analysis of prescribing team activity diary exercise
The number of whole time equivalents deployed to support primary care prescribing (when population adjusted) shows the Health Board has below average staffing levels for Wales (Exhibit 39). However, this is not to say that these levels within the Health Board or Wales are appropriate.
Page 63 of 70 - Primary Care Prescribing - Hywel Dda Health Board
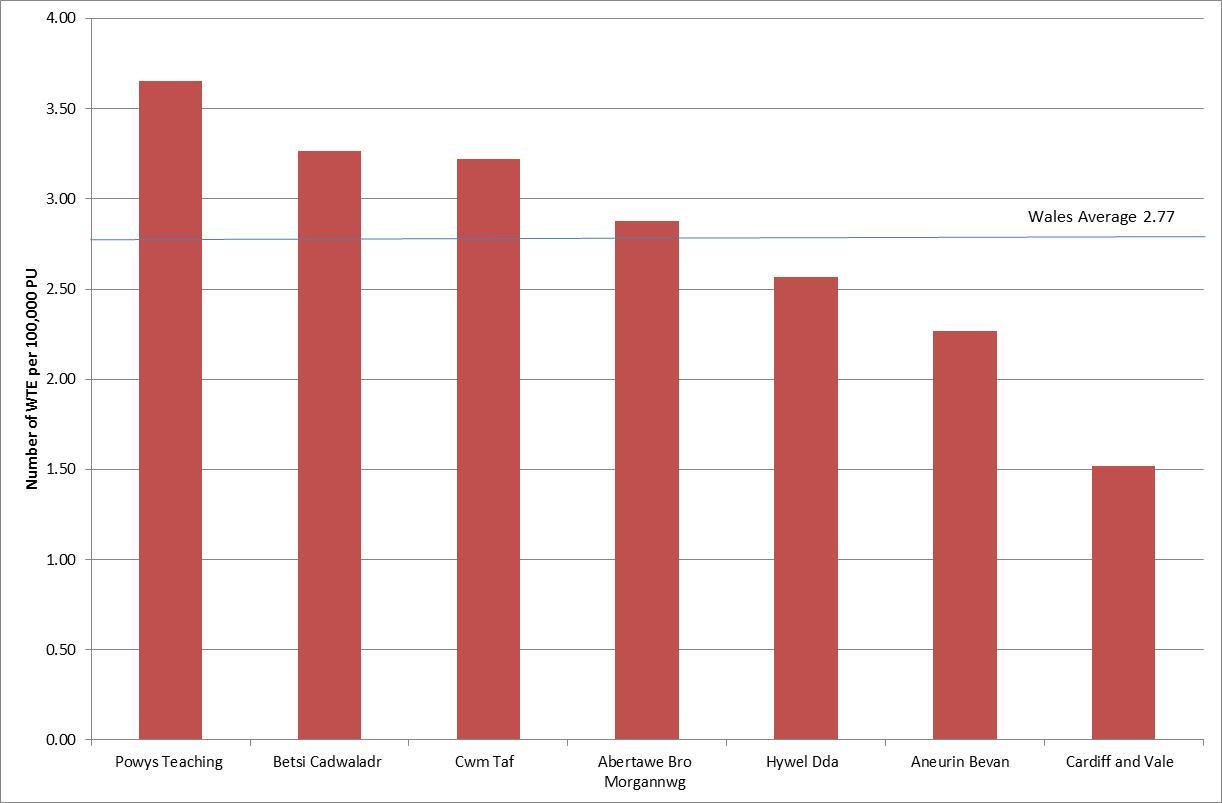
Exhibit 37: Total prescribing support by Health Board
Source: Wales Audit Office analysis of prescribing team activity diary exercise
Exhibit 38: Percentage of time spent by role and key work area
Working in
activities
practices community secondary
care (%
time)
Medicines Management Project Facilitator
Medicines Management Technician
Prescribing Advisor
Prescribing Support Dietician
Prescribing Support Pharmacist
Prescribing Support Technician
Support Functions
Page 64 of 70 - Primary Care Prescribing - Hywel Dda Health Board
Exhibit 39: Activity profile
Activity profile
Percentage
time
Health Board activities
Prescribing or clinical audit and review activities to ensure robust therapeutic /
drug monitoring ensuring safe prescribing of complex drugs.
Supporting / managing the development and maintenance of the LHB formulary.
Providing summaries of MHRA and NPSA warnings that affect medicines for
medical and nursing staff (including audit activity to identify compliance with guidance).
Development of tools to support the management of prescribing.
Development of Medicines Management Local Enhanced Services.
Support and audit relating to the GP contract QoF and Medicines Management
Local Enhanced Services.
Liaison with other healthcare professionals on medicines management issues:
district nurses (eg, wound dressings); dieticians (eg, patient nutrition); local care homes (eg, EMI, nursing and residential) to ensure safe and cost-
effective prescribing of practice patients; and
community pharmacists regarding patient's compliance, waste, prescribing
changes and the management of repeat prescriptions.
Consultations with patients as a prescriber/non-prescriber within areas of
competence eg,diabetes, CVD, COPD/Asthma, pain, Care of the Elderly.
Domiciliary visits for medication review for house-bound patients.
Managing controlled drugs, for example:
controlled drug monitoring; and witnessing destruction of controlled drugs.
Production of newsletters and information for patients / healthcare professionals. 2.8%
Preparation and analysis of CASPA data.
Analysing financial information.
Horizon scanning.
Online script views.
Medicines information enquiries by GPs, nurses, community pharmacists,
patients, locality colleagues, practice staff, MPs/FOI requests.
Attending meetings eg, prescribing team meetings, DTC, LHB primary care
support unit, clinical governance, incident reporting, Dispensing Services, locality meetings, council meetings etc.
Page 65 of 70 - Primary Care Prescribing - Hywel Dda Health Board
Activity profile
Percentage
time
Clinical governance related work.
Risk assessment work.
Travelling time.
Administrative tasks.
Dealing with ADRs.
Working with GP practices.
Reviewing and supporting the management of practices' prescribing budgets
(including interrogation of prescribing data, CASPA).
Training and advising practice staff on:
local and national guidelines (NICE, NSF, DTG decisions; and repeat prescribing systems - improving safety and reducing waste.
Supporting and undertaking clinical audit to identify compliance with guidance.
Supporting practices to manage drug withdrawals and discontinuations of
benzodiazepines.
Promoting cost effective prescribing by utilising medication changes eg,
switches or lower cost equivalent identified under LES 2012-13.
Providing independent advice on the prescribing of novel medicines and sharing
prescribing guidelines within the practice.
Supporting medication reviews in GP practices including:
removal of medicines that have not been issued in the past 12 months; linking medicines to diagnosis and harmonize quantities so that all medicines
fall due at the same time; and
compliance with LHB Medication Review standards.
Promoting and supporting practices to undertake any LHB/WAG initiatives. eg,
1000 Patient Lives Campaign.
Supporting practices about interface prescribing issues.
Supporting the implementation or management of ScriptSwitch.
Training and advising dispensing staff in prescribing practices in completing and
Page 66 of 70 - Primary Care Prescribing - Hywel Dda Health Board
Activity profile
Percentage
time
Working in the community.
Supporting medication reviews:
within local care homes; and for housebound patients.
Providing support to community staff eg, community nurses, district nurses,
heath visitors, case managers, on medicines management queries.
Attending multidisciplinary team meetings within the locality.
Meetings with community pharmacists and other healthcare professionals.
Providing support in care homes, for example:
training for carers; prescription ordering and waste management; MAR sheet completion; controlled drug management; care home medicines management assessment – targeted; and training and advising care home staff in completing and reviewing SOPs.
Providing training for social services staff.
Working with secondary care.
Organising a supply of a hospital-only drug eg, acitretin, dronaderone, clozapine
susp, mercaptopurine, daptomycin injection etc.
Answering queries from GPs regarding a TTO or an OPD letter.
Promoting and supporting LHB/WAG initiatives eg, 1000 Patient Lives
Supporting the safe transcription of medication from hospital:
discharge letters; and targeting specific problem issues.
Developing shared care protocols.
Managing compliance with shared care protocols and RAG system.
Page 67 of 70 - Primary Care Prescribing - Hywel Dda Health Board
European Centre for Disease Prevention and Control (ECDC) key messages for primary care prescribers
Growing antibiotic resistance threatens the effectiveness of antibiotics now and in the future
Antibiotic resistance is an increasingly serious public health problem in Europe.
While the number of infections due to antibiotic-resistant bacteria is growing, the pipeline of new antibiotics is unpromising, thus presenting a bleak outlook on availability of effective antibiotic treatment in the future [3, 4].
Rising levels of antibiotic-resistant bacteria could be curbed by encouraging limited and appropriate antibiotic use in primary care patients
Antibiotic exposure is linked to the emergence of antibiotic resistance. The overall uptake of antibiotics in a population, as well as how antibiotics are consumed, has an impact on antibiotic resistance.
Experience from some countries in Europe shows that reduction in antibiotic prescribing for outpatients have resulted in concomitant decrease in antibiotic resistance.
Primary care accounts for about 80 per cent to 90 per cent of all antibiotic prescriptions, mainly for respiratory tract infections.
There is evidence showing that, in many cases of respiratory tract infection, antibiotics are not necessary and that the patient's immune system is competent enough to fight simple infections.
There are patients with certain risk factors such as, for example, severe exacerbations of chronic obstructive pulmonary disease (COPD) with increased sputum production, for which prescribing antibiotics is needed.
Unnecessary antibiotic prescribing in primary care is a complex phenomenon, but it is mainly related to factors such as misinterpretation of symptoms, diagnostic uncertainty and perceived patient's expectations [14, 21].
Communicating with patients is key
Studies show that patient satisfaction in primary care settings depends more on effective communication than on receiving an antibiotic prescription [22–24] and that prescribing an antibiotic for an upper respiratory tract infection does not decrease the rate of subsequent return visits.
Page 68 of 70 - Primary Care Prescribing - Hywel Dda Health Board
Professional medical advice impacts patients' perceptions and attitude towards their il ness and perceived need for antibiotics, in particular when they are advised on what to expect in the course of the illness, including the realistic recovery time and self-management strategies.
Primary care prescribers do not need to allocate more time for consultations that involve offering alternatives to antibiotic prescribing. Studies show that this can be done within the same average consultation time while maintaining a high degree of patient satisfaction.
Page 69 of 70 - Primary Care Prescribing - Hywel Dda Health Board
Source: https://www.wao.gov.uk/system/files/publications/WAO_Hywel_Dda_Primary_Care_Prescribing_English_2014.pdf
THE VENEER How Indonesia's Last Rainforests are being Felled for Flooring exclusion zone, white area to be kept clear DO NOT PRINT BOX exclusion zone, white area to be kept clear DO NOT PRINT BOX Theft of Indonesia's A Fashion for Flooring Behind the Brand 1. Armstrong/Bruce Executive Summary
GUM DISEASE?? YOU COULD BE AR RISK!! GUM DISEASE Loose Teeth Bleeding Gums Bone Loss Bad Breath & Odor Tartar Buildup Plaque &Bacteria HEALTHY TEETH & GUMS NO Loose Teeth!! NO Bleeding Gums!! NO Bone Loss!!